3519
3D distortion-free diffusion imaging using an accelerated multi-shot diffusion-prepared sequence1Biomedical Engineering, King's College London, London, United Kingdom, 2Siemens Healthcare, Frimley, United Kingdom, 3Cancer Imaging, King's College London, London, United Kingdom
Synopsis
Current methods for cancer diffusion imaging employ 2D single-shot diffusion weighted echo planar imaging sequences, which are fast but have limited resolution and are prone to distortion artefacts. The purpose of this work is to achieve 3D high-resolution and distortion-free diffusion imaging suitable for cancer precision diagnostics and therapy planning. A multi-shot diffusion-prepared sequence with gradient echo readout, centric encoding, and accelerated variable density acquisition was developed and tested in healthy volunteer brains as an exemplar. A full set of 2.2-fold accelerated diffusion weighted images in three diffusion directions was acquired in 4:30 min producing quantitative 3D distortion-free ADC maps.
Introduction
Diffusion-weighted MRI imaging (DWI) is a key component of multi-parametric MRI protocols in cancer imaging for its ability to probe tissue microstructure. Current clinical DWI protocols are based on 2D diffusion-weighted single-shot echo planar imaging (SS-DW-EPI), which is fast, but particularly prone to geometric distortion and of limited spatial resolution. This limits diagnostic accuracy and prohibits its use in emerging MR-guided personalized treatment options, including radiotherapy planning with its high requirement for 3D geometric accuracy.
Multi-shot (MS) sequences can achieve high resolution and have been successfully used for diffusion-weighted imaging of the brain 1,2 (“readout-segmented” EPI, RESOLVE).
MS sequences can be combined with diffusion-preparation (DP) modules (as opposed to diffusion-weighted) 3. DP sequences have the advantage that diffusion-encoding and readout are separated and thus can be optimized independently. Disadvantages include the longer acquisition time.
The purpose of this study is to implement a 3D MS-DP sequence with gradient echo readout (3D DP-MS-GRE) to achieve high-resolution, distortion-free, 3D diffusion using the brain as exemplar.
Methods
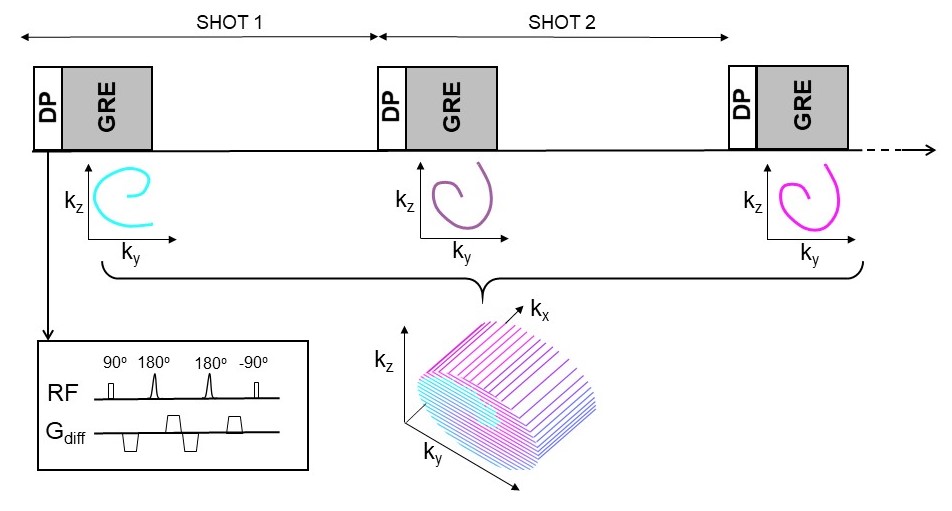
Diffusion sequence. A prototype 3D MS-DP-GRE sequence was implemented. Diffusion preparation is achieved with a twice-refocused spin-echo (TRSE 4) module with a pair of adiabatic refocusing pulses and two pairs of gradients, placed at the beginning of each shot (Figure 1). Data were acquired with a 3D Cartesian k-space trajectory with centric profile order (VD-RAD 5, CASPR 6), both fully sampled (FS) and two-fold (x2.2) prospectively accelerated using a variable density (VD) sampling (Figure 1). Undersampled images were reconstructed in MATLAB using iterative and regularized TV-SENSE reconstruction 7,8.
Experiments. Data were acquired for four healthy subjects on a 3T PET-MR scanner (Biograph mMR, Siemens Healthcare, Erlangen, Germany), following approval by the local institutional review board and informed consent. MR measurements were obtained using 3D MS-DP-GRE with the following acquisition parameters: number of GRE RF pulses per shot = 96, transversal orientation, FA=12o, GRE-TE=4.7ms, FOV=240x240mm2, resolution 1.5x1.5x5mm3, DP-TE=90ms, b-value (diffusion weighting) = 50,800,1200s/mm2, acquisition time (AT) per image=1:06/0:30min (FS/VD), total AT=9:54/4:30min (three diffusion directions for each b-value). To demonstrate the potential of multi-shot diffusion imaging, a higher resolution (1x1x3mm3) MS-DP-GRE dataset was also acquired (total AT=14:34min, FS). As a reference standard to evaluate apparent diffusion coefficient (ADC) quantification, a clinical standard 2D SS-DW-EPI was acquired in transversal orientation, acquired resolution 3x3mm2 (interpolated 1.57x1.57mm2), 5mm slice thickness, b-value = 50, 800, 1500 s/mm2 (2, 5, 15 averages each), total AT=6:45 min. As a reference standard to evaluate geometric distortion, a clinical standard high-resolution 2D T2w TSE was also acquired.
Data analysis. ADC maps were obtained from the trace diffusion images using a standard mono-exponential fitting routine. To compare ADC estimates mean and standard deviation of ADC were measured in manually drawn regions of interest (ROIs) in white matter (WM) and grey matter (GM).
Results
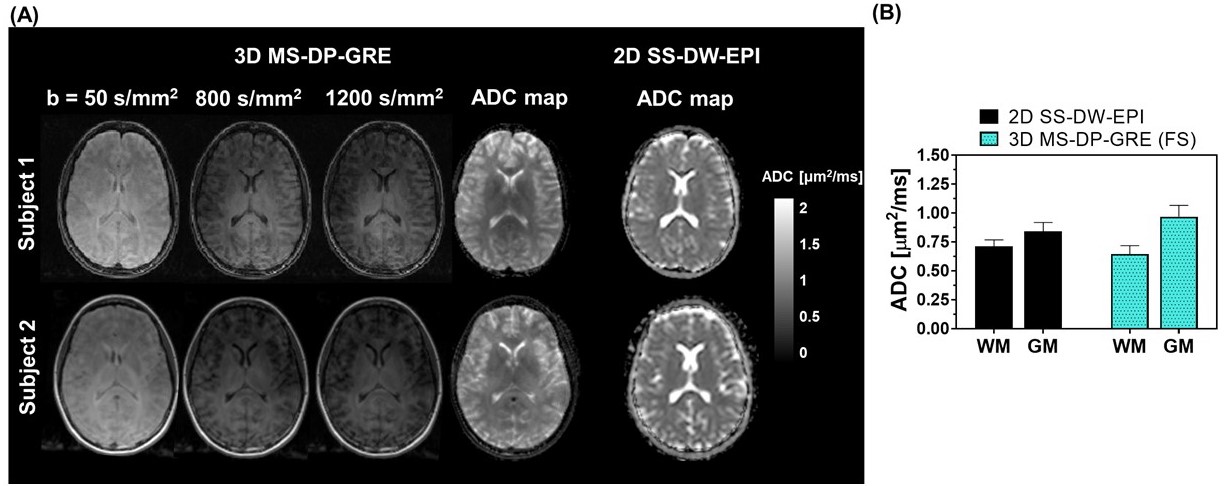
Diffusion images. Trace b-value images obtained with the proposed 3D MS-DP-GRE sequence and corresponding ADC map are shown in Figure 2(A), together with the clinical standard 2D SS-DW-EPI ADC map, for two representative healthy subjects. The MS-DP-GRE-derived ADC values were 0.65±0.07 and 0.97±0.09 μm2/ms for WM and GM respectively (Figure 2(B)), and showed good contrast between WM and GM.
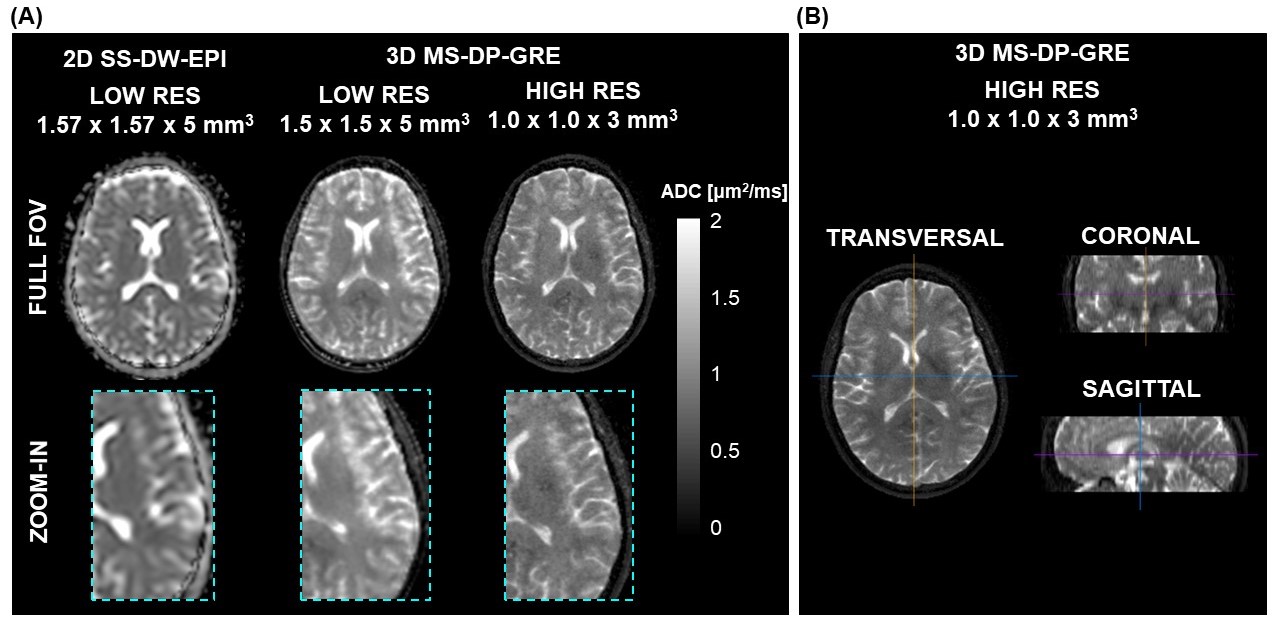
High resolution. ADC maps obtained with the proposed 3D MS-DP-GRE in low and high resolution are shown in Figure 3(A). Reformats in transversal, sagittal and coronal planes of the high-resolution 3D acquisition are shown Figure 3(B).
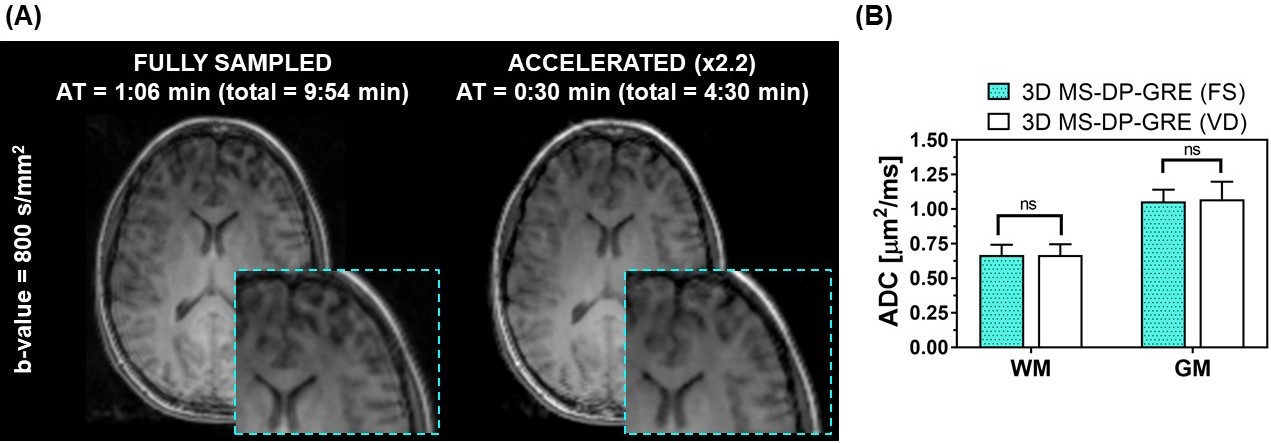
Acceleration. The accelerated acquisition enabled a scan time reduction of 55%. The TV-SENSE reconstructed images showed comparable image quality to the FS, and no statistically significant difference in ADC estimates was observed (Figure 4).
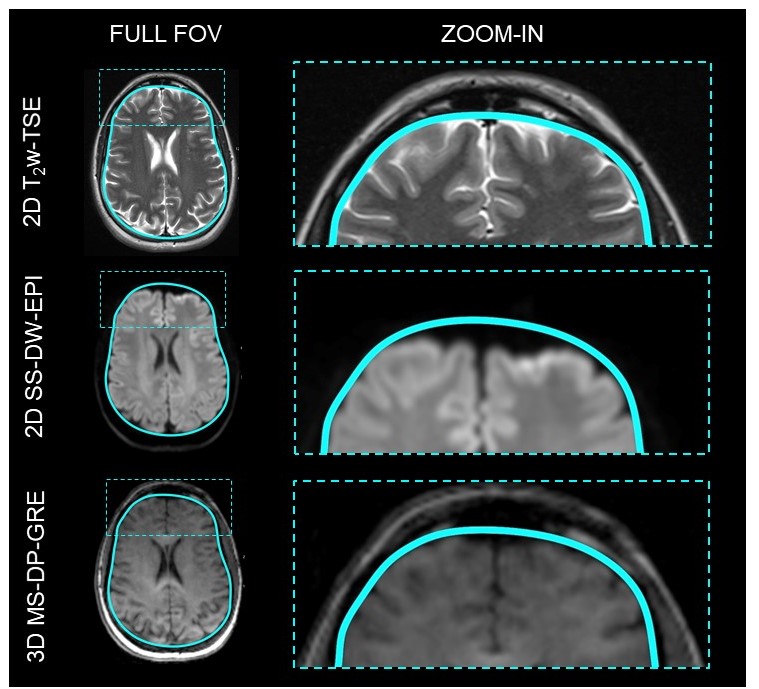
Geometric distortion. With the proposed 3D MS-DP-GRE geometric distortion was substantially reduced compared to the standard 2D SS-DW-EPI using the anatomical 2D T2w-TSE as reference (Figure 5).
Discussion and Conclusion
The
experiments performed in this work show that an accelerated 3D MS-DP-GRE
approach can achieve 3D diffusion mapping with ADC quantification in agreement
with literature values 9,10 and with substantially reduced
distortion in a total acquisition time of 4:30min. This should prove useful for
MR-guided focal therapy and interventions, including MR-guided radiotherapy
planning.
Future work will address the motion sensitivity
of the multi-shot approach, i.e. image corruption due to inter-shot motion and
phase incoherence, to enable robust ADC quantification also in motion-affected
organs.Acknowledgements
This work was supported by the King’s College London & Imperial College London EPSRC Centre for Doctoral Training in Medical Imaging [EP/L015226/1]; the Wellcome EPSRC Centre for Medical Engineering at Kings College London [WT 203148/Z/16/Z]; the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London; the King’s Health Partners Research and Development Challenge Fund; TOHETI; NIHR BRC; GSTT/KCL BRC; CRUK/EPSRC Cancer Centre; Siemens Healthineers. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. O’Halloran RL, Aksoy M, Van AT, Bammer R. 3D isotropic high-resolution diffusion-weighted MRI of the whole brain with a motion-corrected steady-state free precession sequence. Magn Reson Med. 2013;70(2):466-478.
2. Madore B, Chiou JYG, Chu R, Chao TC, Maier SE. Accelerated multi-shot diffusion imaging. Magn Reson Med. 2014;72(2):324-336.
3. Nguyen C, Fan Z, Sharif B, et al. In vivo three-dimensional high resolution cardiac diffusion-weighted MRI: A motion compensated diffusion-prepared balanced steady-state free precession approach. Magn Reson Med. 2014;72(5):1257-1267.
4. Reese TG, Heid O, Weisskoff RM, Wedeen VJ. Reduction of eddy-current-induced distortion in diffusion MRI using a twice-refocused spin echo. Magn Reson Med. 2003;49(1):177-182.
5. Cheng JY, Zhang T, Ruangwattanapaisarn N, et al. Free-Breathing Pediatric MRI with Nonrigid Motion Correction and Acceleration. J Magn Reson Imaging. 2015;42(2):407-420.
6. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015;41(3):738-746.
7. Tamir JI, Ong F, Cheng JY, Uecker M, Lustig M. Generalized Magnetic Resonance Image Reconstruction using The Berkeley Advanced Reconstruction Toolbox. In: ISMRM Workshop on Data Sampling and Image Reconstruction. 2016.
8. Cruz G, Atkinson D, Buerger C, Schaeffter T, Prieto C. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. Magn Reson Med. 2016;75(4):1484-1498.
9. Helenius J, Soinne L, Perkiö J, et al. Diffusion-weighted MR imaging in normal human brains in various age groups. Am J Neuroradiol. 2002;23(2):194-199.
10. Grech-Sollars M, Hales PW, Miyazaki K, et al. Multi-centre reproducibility of diffusion MRI parameters for clinical sequences in the brain. NMR Biomed. 2015;28(4):468-485.
Figures