3516
TRACTOGRAPHY OF THE TRIGEMINAL NERVE OUTSIDE THE BRAIN1SBHSE, Arizona state university, Tempe, AZ, United States
Synopsis
Diffusion Tensor Imaging (DTI) tractography used for the visualization of cranial nerves has mostly focused on tracts inside the brain. This work focuses on tracking trigeminal nerve branches using DTI outside the brain. Trigeminal nerve efferents in the face can be stimulated using transdermal electrical neuromodulation. Locations of subcutaneous tracts of the ophthalmic and maxillary branches of the trigeminal nerve may assist with electrode placement in these studies. Here, we describe use of HARDI-derived DTI to determine locations of trigeminal nerve projections in the face.
INTRODUCTION
Determination of trigeminal nerve efferent location is a critical step in studying peripheral trigeminal nerve stimulation (TNS) in humans. The trigeminal nerve exits the skull via the supraorbital, infraorbital and mental foramina as the ophthalmic, maxillary and mandibular branches, respectively, into the face. The trigeminal nerve transmits sensory information from the face via monosynaptic connections to the trigeminal sensory nuclear complex (TSNC) in the brain. The TSNC sends sensory information to multiple brain regions that regulate arousal and coordinate neurobehavioral engagement with the environment[1]. Neuromodulation of TSNC can be achieved through non-invasive and safe transdermal neurostimulation methods and can be studied by measuring flow of current in and around the scalp through magnetic resonance electrical impedance tomography (MREIT)[2]. For successful transdermal electrical stimulation of trigeminal nerve, stimulating electrodes must be placed in accurate locations on the face. Previous DTI tractography research has only tracked the trigeminal nerve in the cisternal region inside the brain[3-5]. This study uses probabilistic tractography of the trigeminal nerve outside the brain to follow it from the brainstem to the face.METHODS
A 3T MRI scanner (Philips Ingenia System, Barrow Neurological Institute, Phoenix, USA) was used to obtain 3D T1-weighted images and diffusion images of a single female human subject using a 32-channel head coil. All procedures were performed in accordance with Arizona State University IRB guidelines. A high-resolution 3D FLASH T1-weighted structural image was acquired with a 240 mm (FH) × 240 mm (AP) × 200 mm (RL) field-of-view (FOV) and 1 mm isotropic resolution. A HARDI (high angular resolution diffusion imaging) protocol[6] was followed for diffusion weighted MR (DWI) data acquisition. Data was collected at b-values of 100 s/mm2 (6 directions) and 1000 s/mm2 (64 directions) with 2 mm isotropic resolution and matrix size of 240mm × 240mm × 100mm. Two 6-direction DWI data sets were gathered with reversed phase encode directions to remove effects of background eddy currents.
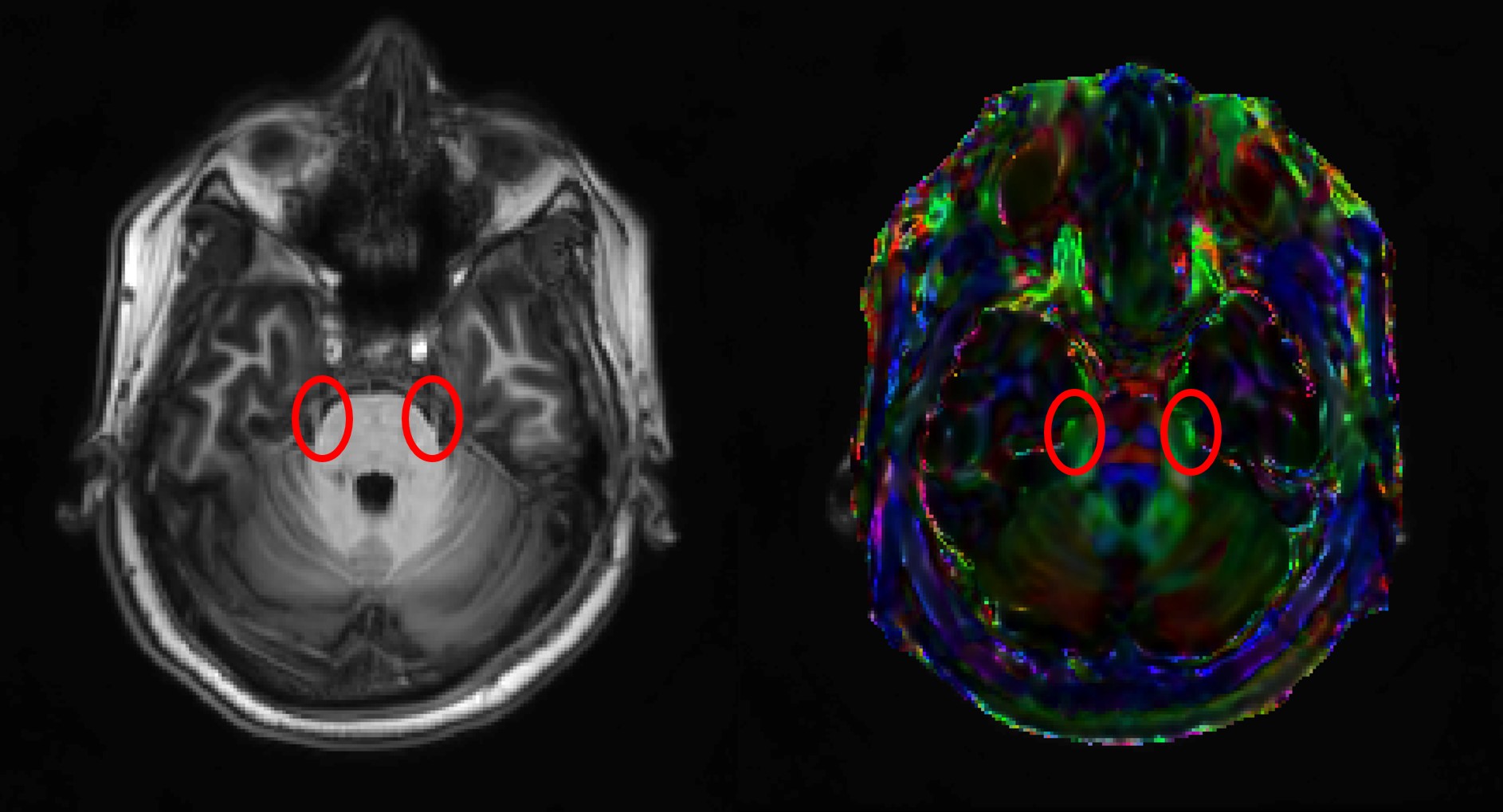
The diffusion data was processed using FMRIB Software Library (https://fsl.fmrib.ox.ac.uk/fsl). The processing involved converting DICOM images to NIfTI format, removal of magnetic inhomogeneity effects using the FSL topup procedure[7] and fitting tensor models using the FSL bedpostX function (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FDT/UserGuide). A downsampled T1-weighted image was co-registered with diffusion images to help place seed masks and waypoint tract guiding masks. Each branch of the trigeminal nerve was tracked separately. The same seed mask was placed bilaterally on the starting point of the trigeminal nerve from brainstem in the locus coerulus structure as identified on the T1- weighted volume (Fig. 1) for each tract. Waypoint masks were placed bilaterally at the supraorbital foramen for the ophthalmic branch and at the infraorbital foramen for the maxillary branch. Probabilistic fiber tracking was performed using FSL’s probtrackX function. The number of samples was set at 40000, curvature threshold was 0.2 with loop check on and step size was set at 2 mm, to match the acquisition voxel resolution.
RESULTS AND DISCUSSION
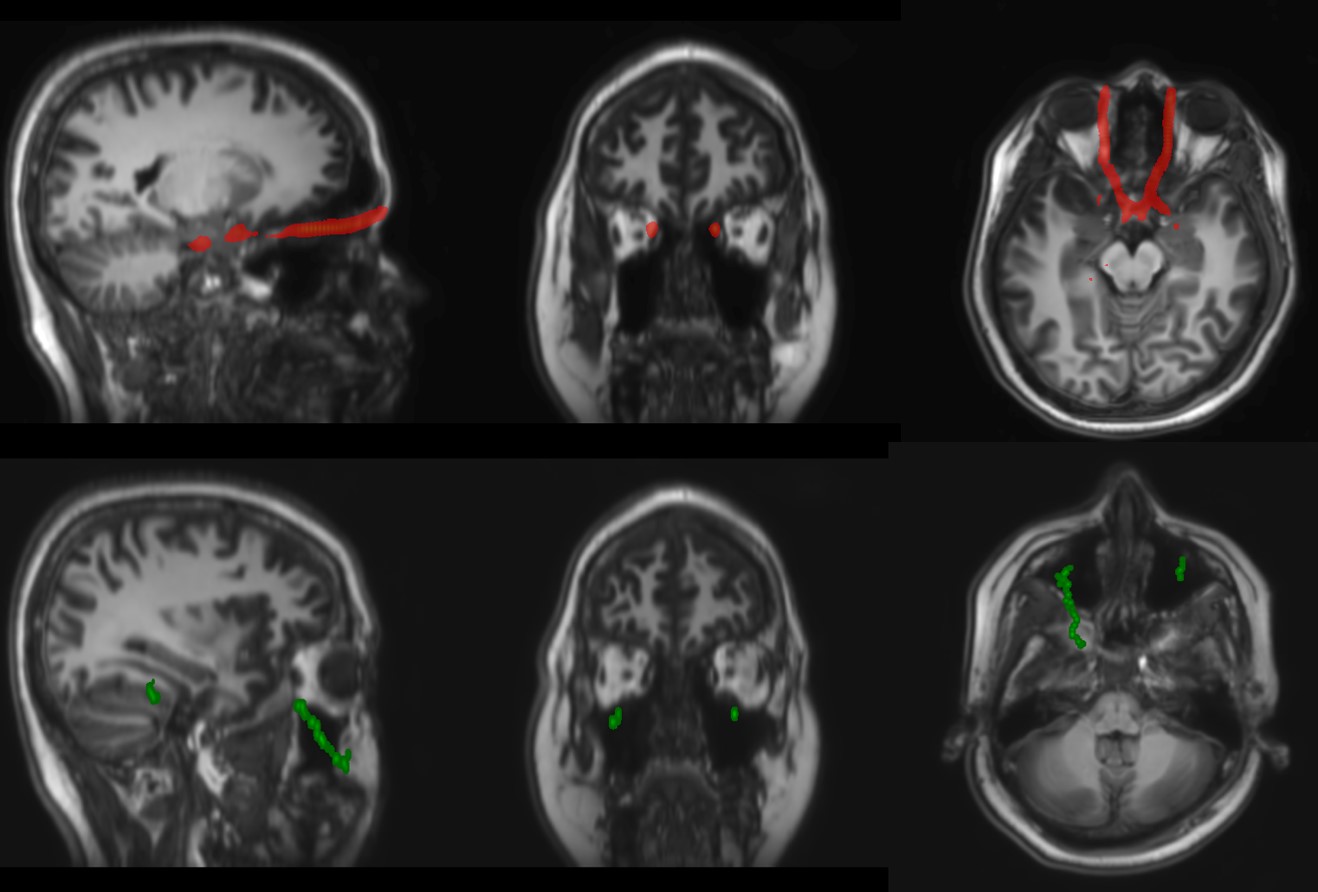
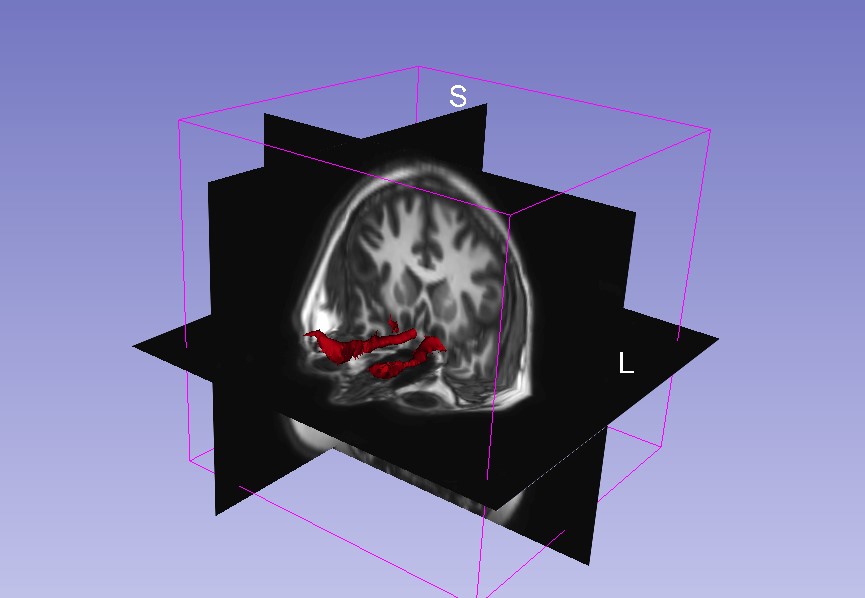
The tracts were obtained individually and thresholded to visualize the nerves of interest (Fig. 2).
The opthalmic branch was successfully tracked from brainstem to the face and was symmetric. Tracts were also observed in the maxillary branch, but were not symmetric. This could be due to error in waypoint mask placement or reflect actual asymmetries. In future work, tracts for the mandibular branch of the trigeminal nerve will be explored. These tractography analyses will be extended to include other data obtained using this protocol to validate these findings.
CONCLUSION
We identified two branches of trigeminal nerve tracts extending to the face. This information will be used to inform electrode placement used in trigeminal nerve neurostimulation. The knowledge of trigeminal nerve location will also help assist MREIT data analysis during neuromodulation experiments. This also establishes grounds for the robustness of HARDI-DTI protocol to track nerves outside the brain.Acknowledgements
This work was supported by Defense Advanced Research Projects Agency (DARPA) award N66001-17-2-4018 to SHT.References
1. L. Bradnam and C. Barry, “The Role of the Trigeminal Sensory Nuclear Complex in the Pathophysiology of Craniocervical Dystonia,” J. Neurosci., vol. 33, no. 47, pp. 18358–18367, 2013.
2. A. K. Kasinadhuni, A. Indahlastari, M. Chauhan, M. Schär, T. H. Mareci, and R. J. Sadleir, “Imaging of current flow in the human head during transcranial electrical therapy,” Brain Stimul., vol. 10, no. 4, pp. 764–772, 2017.
3. M. Yoshino et al., “Visualization of cranial nerves using high-definition fiber tractography,” Neurosurgery, vol. 79, no. 1, pp. 146–165, 2016.
4. K. A. Cauley and C. G. Filippi, “Diffusion-tensor imaging of small nerve bundles: Cranial nerves, peripheral nerves, distal spinal cord, and lumbar nerve roots- Clinical applications,” Am. J. Roentgenol., vol. 201, no. 2, 2013.
5. A. Rousseau et al., “Diffusion tensor magnetic resonance imaging of trigeminal nerves in relapsing herpetic keratouveitis,” PLoS One, vol. 10, no. 4, 2015.
6. M. Chauhan, A. Indahlastari, A. K. Kasinadhuni, M. Schar, T. H. Mareci, and R. J. Sadleir, “Low-Frequency Conductivity Tensor Imaging of the Human Head In Vivo Using DT-MREIT: First Study,” IEEE Trans. Med. Imaging, vol. 37, no. 4, pp. 966–976, 2018.
7. J. L. R. Andersson, S. Skare, and J. Ashburner, “How to correct susceptibility distortions in spin-echo echo-planar images: Application to diffusion tensor imaging,” Neuroimage, vol. 20, no. 2, pp. 870–888, 2003.
Figures