3502
Towards clinically viable and robust measurement of microscopic diffusion anisotropy1Department of Medical Biophysics, Schulich School of Medicine and Dentistry, University of Western Ontario, London, ON, Canada, 2Centre for Functional and Metabolic Mapping, Robarts Research Institute, Western University, London, ON, Canada
Synopsis
In contrast to fractional anisotropy, microscopic diffusion anisotropy allows measurement of pore structural anisotropy with no influence from orientational coherence. However, acquisitions that allow in vivo measurement of microscopic anisotropy are generally time-consuming and/or low SNR. Here, we introduce an efficient approach to perform isotropic diffusion encoding and measure high quality full-brain microscopic anisotropy in a scan time of only 3 minutes at 7T. Results are demonstrated in a healthy subject and MS patient, where clear delineation of lesions is observed in the latter case.
Introduction
Diffusion MRI (dMRI) gives insight into neuronal integrity via metrics such as fractional anisotropy (FA) and mean diffusivity.1 FA describes the degree of diffusion anisotropy within tissue but cannot distinguish between neuron integrity and fiber orientation coherence. In contrast, microscopic anisotropy (µA) and microscopic fractional anisotropy (µFA) are sensitive to diffusion anisotropy independent of neuron fiber orientation.2
To date, most in vivo demonstrations of µA have been time-consuming and/or low SNR. Here, we demonstrate a new isotropic encoding scheme and µA protocol that requires a clinically feasible scan time of only 3 minutes for full-brain coverage on a 7T head-only MRI.
Methods
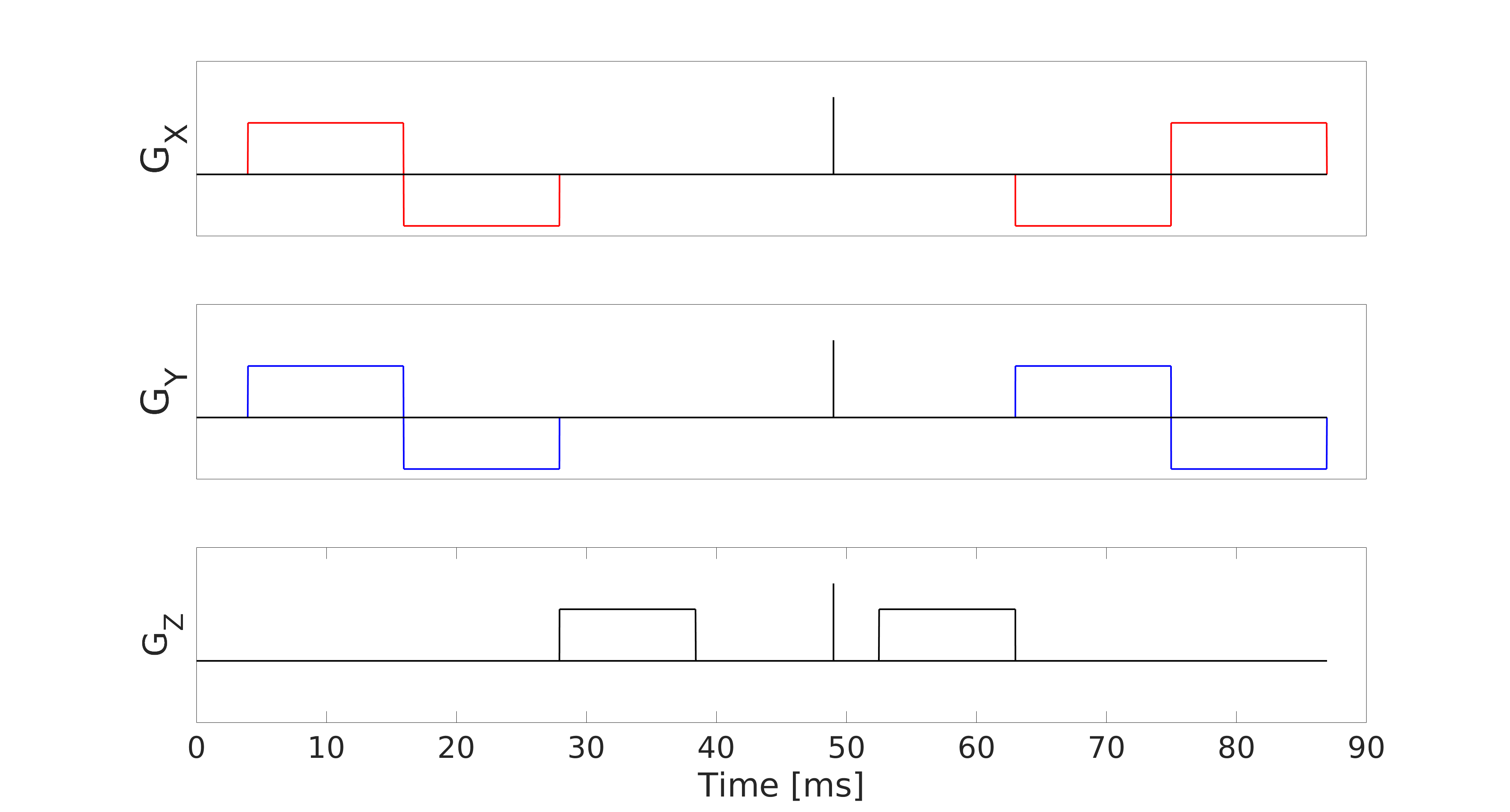
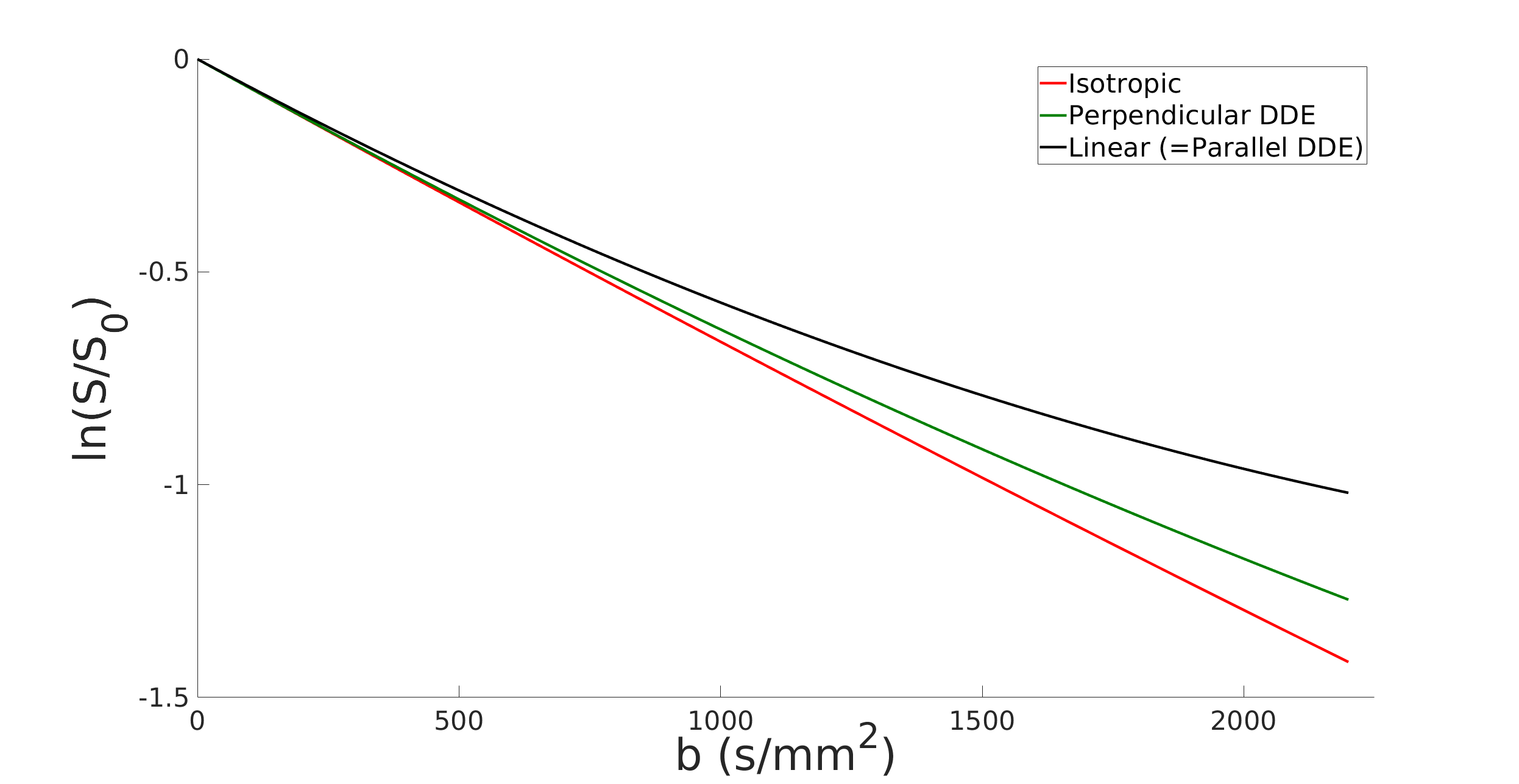
Data was collected from a healthy volunteer and a relapsing-remitting multiple sclerosis (MS) patient, abiding by ethics board guidelines, on a 7T head-only MRI system (80 mT/m strength and 350 T/m/s slew rate) using 7, 15, and 30 linear encodings at b = 100 s/mm2, 1000 s/mm2, and 2200 s/mm2, respectively. The same number of isotropic encodings were acquired at each b-value. The other parameters were TE/TR = 99/6000 ms, FOV = 196x196 mm2, 2 mm isotropic in-plane resolution, 36 slices (4 mm), R=2 GRAPPA, 10.5 min scan time. Post-processing included PCA denoising 3 and eddy current correction with FSL.4 To encode diffusion isotropically, we developed an efficient method that utilizes trapezoidal gradients (Fig. 1) (e.g., FAMED 5 would achieve only b = 1150 s/mm2 in the same TE). Isotropic encoding was chosen over double diffusion encoding (DDE) because there is greater contrast between linear and isotropic encoded diffusion-weighted signals than between linear and perpendicular DDE signals (Monte Carlo simulation 6; Fig. 2). Notably, the proposed scheme requires approximately the same TE as multi-directional DDE would to achieve to the same b-value.
To assess feasibility of a rapid clinical scan, the full data set was subsampled to only 15 linear directions and 15 isotropic acquisitions (both at b = 2200 s/mm2) before computing µA via 7:$$\mu A^2= b^{-2}[ln(S_{linear})-ln(S_{isotropic})]$$where Slinear and Sisotropic are the powder averages of the linear and isotropic scans, respectively. The 15 linear directions with b = 1000 s/mm2 were used to compute FA maps for comparison, and a dual-inversion recovery (DIR) acquisition was performed on the MS patient to identify lesions.
Results
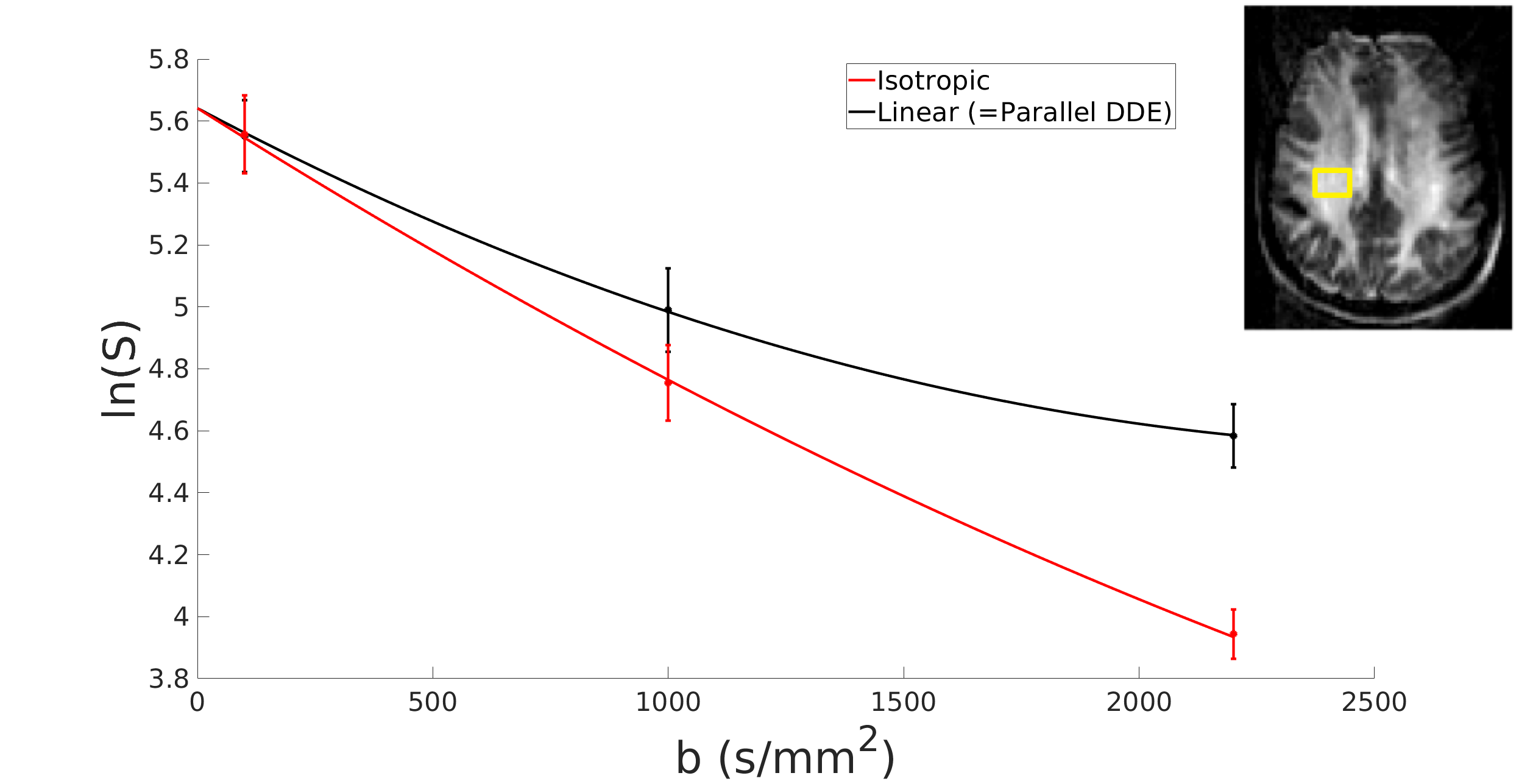
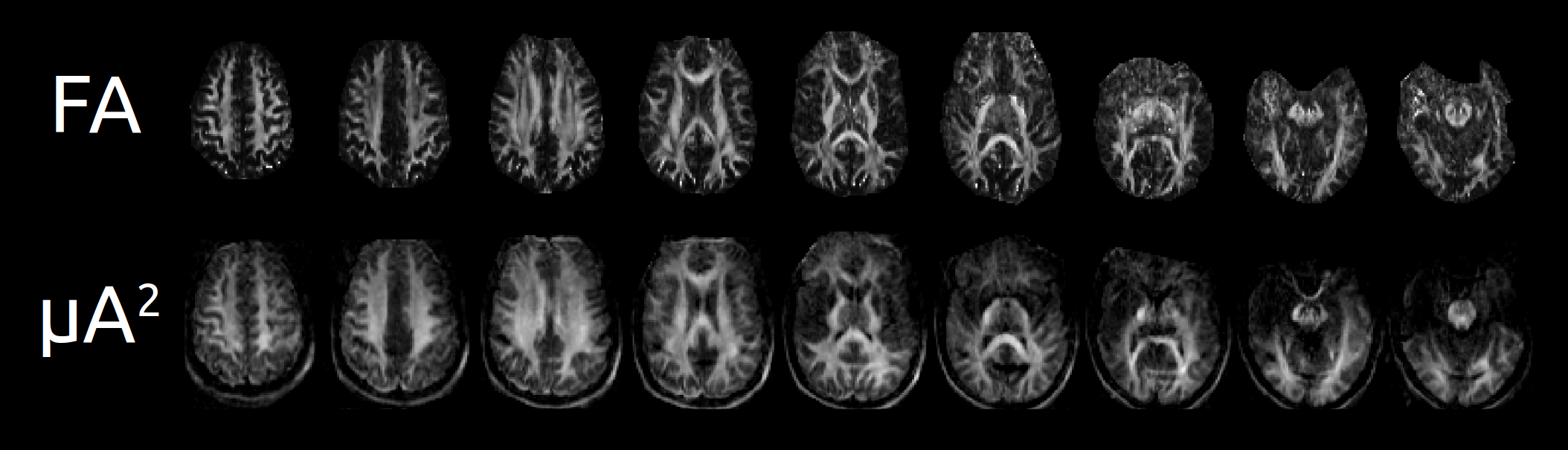
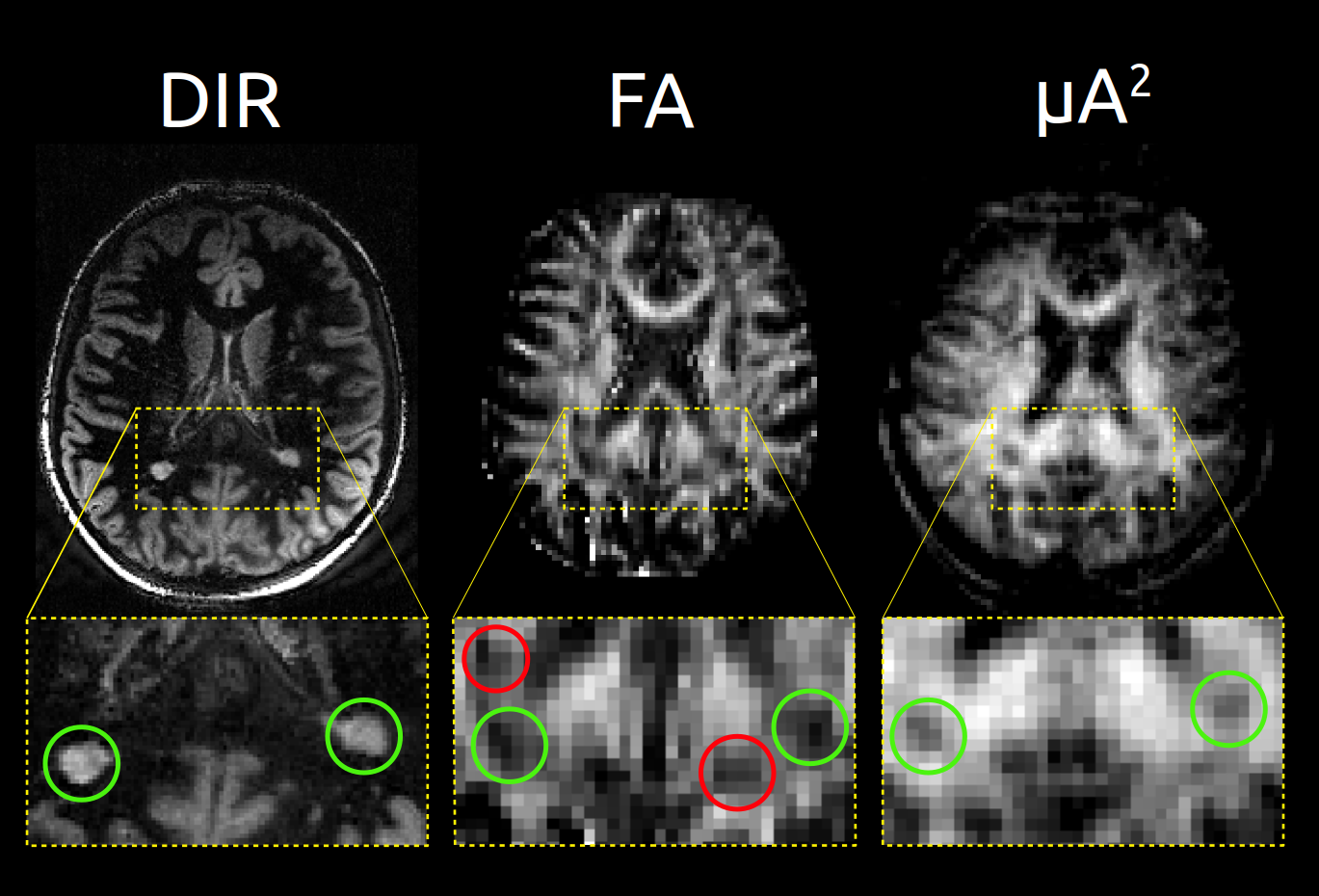
Signal trends in a region of interest (from the full data set) reflect typical behaviour for linear versus isotropic encoding 8 (Fig. 3). In the healthy subject (subsampled data sets), hypointense regions can be observed in the white matter (WM) on FA but not µA2, suggestive of crossing neuron fibers (Fig. 4). In the MS patient (subsampled data sets), hyperintense WM lesions on the DIR image correspond to hypointensities on FA and µA2 , showing that both metrics are sensitive to MS lesions (Fig. 5). However, additional hypointense regions are observed in the FA map that do not correspond to lesions in µA2 or T2-DIR.Discussion
The subsampled data used to generate the images in Figs 4 and 5 would only require 3 min scan time, demonstrating high feasibility for clinical µA measurements. At TE = 99 ms, the SNR advantages of 7T over 3T were modest and similar quality images may be feasible at 3T with 80mT/m gradients.
The sensitivity of µA to MS lesions is comparable to recent work using DDE at 3T by Yang 9. Here, the higher gradient and field strength and thicker slices reduced the required TE, reduced scan time, increased brain coverage, and improved in-plane resolution. The extent to which the increased contrast for isotropic encoding relative to DDE (i.e., Fig. 2) improved quality remains to be determined.
Methods published to date to compute µA or µFA in vivo using isotropic encoding have involved fitting the diffusion-weighted signal to a constrained model 8, which allows estimation of both µFA and size heterogeneity. While the approach used here only allows computation of an “apparent” µA, it has less stringent acquisition requirements and can be rapidly computed with no need for tuning/regularization, which is essential for practical clinical use.
Future work will aim to adapt these methods to a clinical MRI system and to further investigate the relationship between µA and MS pathology.
Acknowledgements
Canada First Research Excellence Fund to BrainsCAN
Ontario Graduate Scholarships
References
1. Basser, P. J., Mattiello, J. & LeBihan, D. MR diffusion tensor spectroscopy and imaging. Biophys. J. 66, 259–267 (1994).
2. Shemesh, N. et al. Conventions and nomenclature for double diffusion encoding NMR and MRI. Magn. Reson. Med. 75, 82–87 (2016).
3. Veraart, J. et al. Denoising of diffusion MRI using random matrix theory. Neuroimage 142, 394–406 (2016).
4. Andersson, J. L. R. & Sotiropoulos, S. N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage 125, 1063–1078 (2016).
5. Vellmer, S. et al. Comparative analysis of isotropic diffusion weighted imaging sequences. J. Magn. Reson. 275, 137–147 (2017).
6. Hall, M. G. & Alexander, D. C. Convergence and parameter choice for Monte-Carlo simulations of diffusion MRI. IEEE Trans. Med. Imaging 28, 1354–1364 (2009).
7. Ianuş, A., Shemesh, N., Alexander, D. C. & Drobnjak, I. Double oscillating diffusion encoding and sensitivity to microscopic anisotropy. Magn. Reson. Med. 78, 550–564 (2017).
8. Szczepankiewicz, F. et al. The link between diffusion MRI and tumor heterogeneity: Mapping cell eccentricity and density by diffusional variance decomposition (DIVIDE). Neuroimage 142, 522–532 (2016).
9. Yang, G., Tian, Q., Leuze, C., Wintermark, M. & McNab, J. A. Double diffusion encoding MRI for the clinic. Magn. Reson. Med. (2017). doi:10.1002/mrm.27043
Figures