3493
Oscillating Gradient Spin-Echo Diffusion Tensor Imaging of the Human Brain using FLAIR1Biomedical Engineering, University of Alberta, Edmonton, AB, Canada, 2Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Oscillating-gradient spin-echo (OGSE) diffusion tensor MRI permits very short diffusion times (e.g. 5 ms) relative to the typical pulsed-gradient spin-echo (PGSE), but it is challenging to acquire in the human brain. Given low b-values and spatial resolution, it is more prone to problematic artifacts such as Gibbs ringing and partial-volume effects that can compromise diffusion parameter measurements. It is shown here that the use of inversion-recovery FLAIR to suppress cerebrospinal fluid can significantly reduce such artifacts, improve overall image/map quality, and provide better quantitation of OGSE-PGSE diffusion parameter differences in the white matter of the human brain.
Introduction
Oscillating-gradient spin-echo (OGSE) diffusion MRI enables much shorter diffusion times (e.g. 5 ms) that can provide insight into the scale of micro-structural restrictions when compared to conventional pulsed gradient spin echo (PGSE) with longer diffusion times (e.g. 40 ms). OGSE can only be acquired at low b-values (e.g. 200-300 s/mm2 previously) and limited spatial resolution in human brain,1,2 making them sensitive to noise and artifacts such as Gibbs ringing and partial-volume effects. These effects are more problematic given the very small differences of diffusivity parameters seen/expected over this diffusion time range. Although suppression of cerebrospinal fluid (CSF) using FLAIR has long been known to reduce partial-volume effects in diffusion MRI,3,4 it could also remove Gibbs ringing a priori in acquisition by eliminating the bright CSF/brain boundary on b0 images, rather than relying on post-processing.5,6 The purpose here was to investigate the utility of FLAIR for OGSE diffusion tensor imaging (DTI) in the human brain.Methods
PGSE and OGSE DTI with and without FLAIR preparation (inversion time TI 2300 ms) were acquired in five healthy adults (32±9 years, 2 females) on a 3T MAGNETOM Prisma with a 64-channel head coil (Siemens Healthcare, Erlangen, Germany) using a prototype 2D ss-EPI sequence with: GRAPPA 2, 10 3 mm axial slices, 3 mm interslice gap, 1.7x1.7 mm2 in-plane resolution zero-filled to 0.85x0.85 mm2, FOV 220 mm, 128x128 acquisition matrix, and 6 diffusion-encoding directions of b-value 500 s/mm2 (both chosen to minimize TE and retain signal). PGSE used the same TE/TR/scan time as OGSE, but more averages were acquired for FLAIR to account for SNR loss: standard non-FLAIR DTI- 3 averages, TE 78 ms, TR 5600 ms, 2:24 min scan time; FLAIR DTI- 5 averages, TE 93 ms, TR 7400 ms, 4:53 min scan time. PGSE had a typical diffusion time of 40 ms whereas OGSE used trapezoid cosines at 40 Hz with a very short diffusion time of 5.1 ms. Standard preprocessing including Gibbs ringing correction (TV on non-DWI) was performed (ExploreDTI) followed by manual ROI-based measurement (ITK-Snap) of fractional anisotropy (FA) and mean (MD), axial (AD), and radial (RD) diffusivities of the central portions of 3 white matter regions, namely the genu (gCC) and splenium of corpus callosum (sCC) and posterior limb of internal capsule (PLIC), on a single slice to compare OGSE-PGSE for non-FLAIR and FLAIR acquisitions.Results
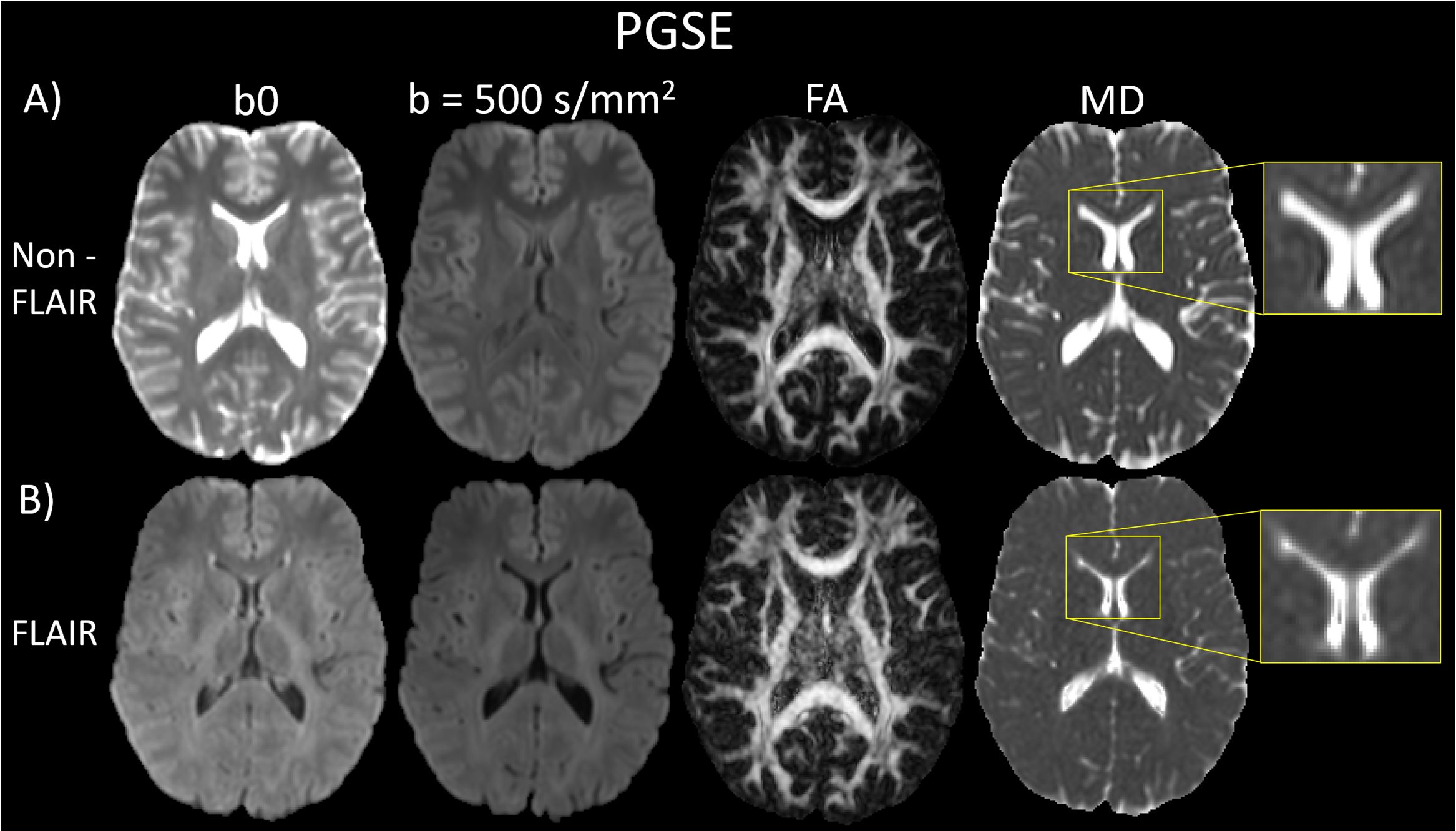
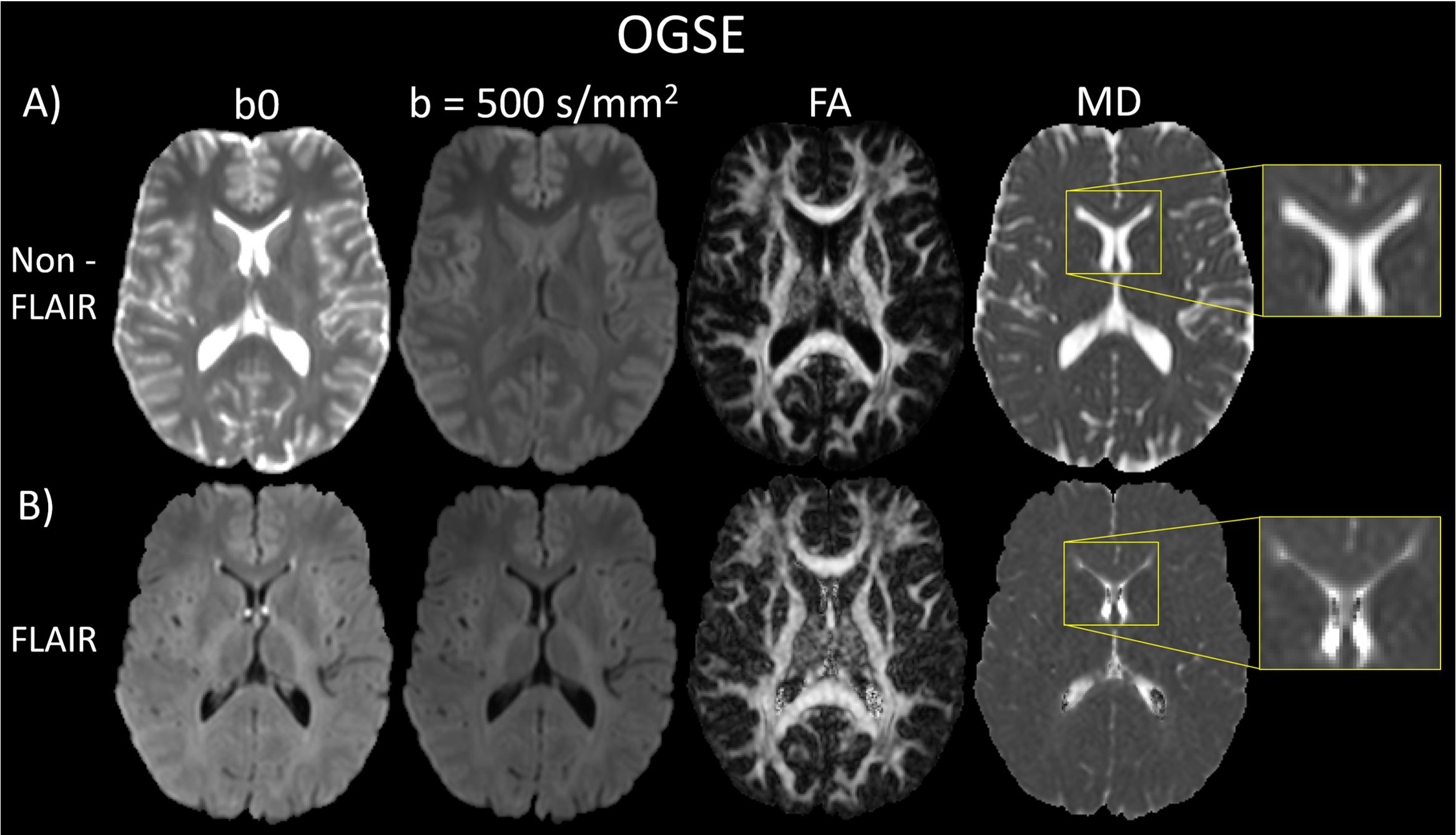
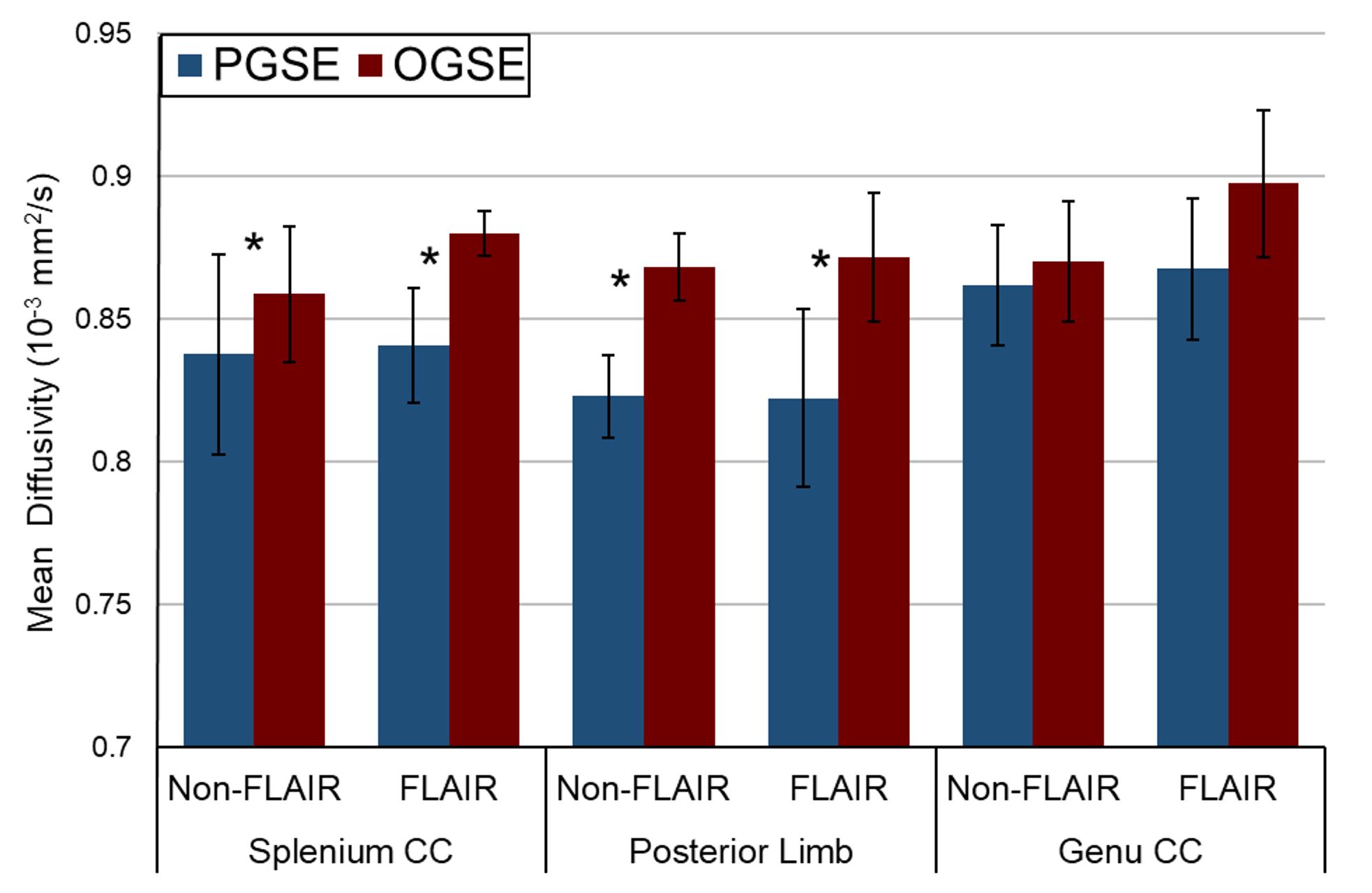
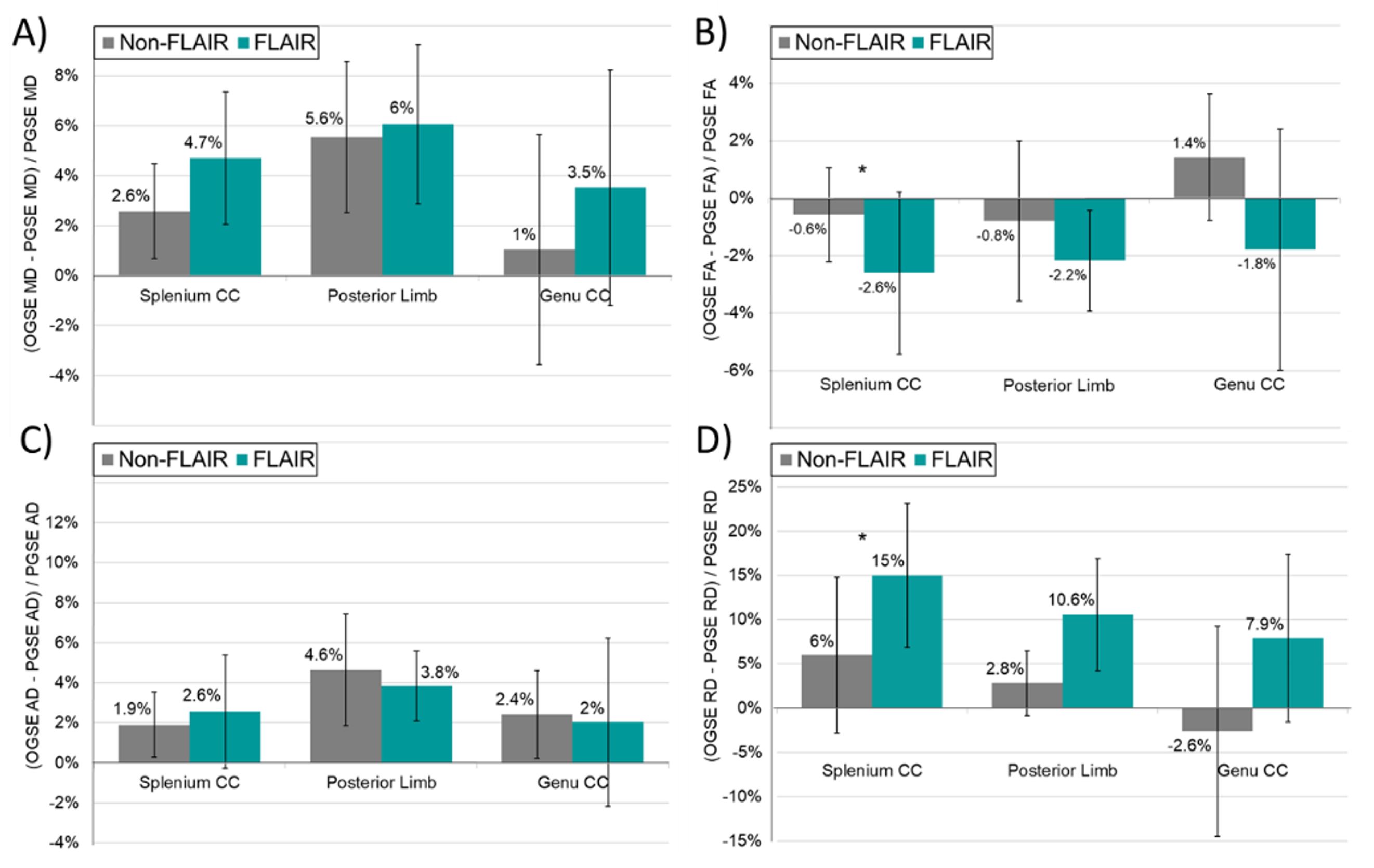
The standard non-FLAIR DTI on both PGSE and OGSE shows focal artifacts on the MD maps due to Gibbs ringing in regions near CSF, for example the zoomed-in region of the genu and lateral ventricles, despite the use of Gibbs ringing correction in post-processing (Figure 1A, 2A). The use of FLAIR for attenuating the CSF signal on the b0 images (and an additive effect with diffusion-weighting on the b500 images) leads to the expected uniform MD maps, as well as good-quality FA maps, for both PGSE and OGSE (Figure 1B, 2B). As expected, the MD from the shorter-diffusion-time OGSE is greater than that derived from the longer-diffusion-time PGSE for the splenium and posterior limb for both non-FLAIR and FLAIR acquisitions, but the genu did not show OGSE-PGSE MD differences on either one (Figure 3). Although the OGSE-PGSE MD differences of ~5-6% were similar between non-FLAIR and FLAIR for splenium and posterior limb (Figure 4A), FLAIR-DTI showed more consistent lower FA (Figure 4B) and elevated RD with OGSE (Figure 4D) particularly in the splenium. At short diffusion times, RD is expected to increase by a greater extent than AD due to greater restrictive effects perpendicular to the axons than parallel. This was observed in all 3 tracts for the FLAIR-DTI acquisition where OGSE RD was increased by 15% (sCC), 11% (PLIC), and 8% (gCC) compared to AD increases of 2-4% (Figure 4C). In contrast, the standard non-FLAIR DTI had limited RD increases of 6% (sCC), 3% (PLIC), and -3% (gCC) where only one was greater than AD.Discussion and Conclusions
OGSE and PGSE diffusion tensor imaging is challenging to acquire in the human brain. The use of inversion-recovery FLAIR to suppress CSF signal greatly increases their image quality and diffusion map accuracy by reducing artifacts such as Gibbs ringing and minimizing partial-volume effects on quantitation. The obvious trade-off is lower SNR (although still more than adequate) and longer scan time due to the inversion and delay. Such OGSE acquisition improvements provide more robust identification of the small, but present, diffusion parameter differences as a function of shorter diffusion times that can provide insight into microstructural scale differences across white matter tracts and with pathology.Acknowledgements
No acknowledgement found.References
[1] Van AT, Holdsworth SJ, Bammer R. In vivo investigation of restricted diffusion in the human brain with optimized oscillating diffusion gradient encoding. Magn Reson Med 71, 83 (2014).
[2] Baron C, Beaulieu C. Oscillating gradient spin echo (OGSE) diffusion tensor imaging of the human brain. Magn Reson Med 72, 726 (2014).
[3] Kwong KK, McKinstry RC, Chien D, Crawley AP, Pearlman JD, Rosen BR. CSF-suppressed quantitative single-shot diffusion imaging. Magn Reson Med 21, 157 (1991).
[4] Papadakis NG, Martin KM, Mustafa MH, Wilkinson ID, Griffiths PD, Huang CL, Woodruff PW. Study of the effect of CSF suppression on white matter diffusion anisotropy mapping of healthy human brain. Magn Reson Med 48, 394 (2002).
[5] Perrone D, Aelterman J, Pižurica A, Jeurissen B, Philips W, Leemans A. The effect of Gibbs ringing artifacts on measures derived from diffusion MRI. Neuroimage 120, 441 (2015).
[6] Veraart J, Fieremans E, Jelescu IO, Knoll F, Novikov DS. Gibbs ringing in diffusion MRI. Magn Reson Med 76, 301 (2016).
Figures