3489
Silent Distortionless DWI1Radiology, Stanford University, Stanford, CA, United States, 2Electrical Engineering, Stanford University, Stanford, CA, United States, 3GE Healthcare, Menlo Park, CA, United States, 4Pediatric Radiology, Lucile Packard Children’s Hospital, Stanford University, Stanford, CA, United States, 5Electrical Engineering and Computer Science, UC Berkeley, Berkeley, CA, United States
Synopsis
Standard clinical EPI based diffusion sequence has high acoustic noise, which is uncomfortable for patients. The images acquired by single-shot EPI also suffer from distortion in areas of large susceptibility variations. To overcome these two limitations, we have developed a silent and distortion-free DWI sequence using a driven equilibrium diffusion prepared multi-segmented Rotating Ultra-Fast Imaging Sequence (RUFIS) readout. The sequence was validated in phantom, volunteers, and patients. The results showed the proposed sequence provides similar diffusion contrast and ADC measurement compared to DW-EPI, with improved image quality and a sound level that approaches that of ambient noise.
Introduction
Standard clinical diffusion-weighted echo planar imaging (DW-EPI) has high acoustic noise, which is uncomfortable for patients, especially pediatric patients. The images acquired by single-shot EPI also suffer from image distortion in areas of large susceptibility variations. To overcome these two limitations, we aim to develop a silent and distortion-free DWI sequence.Methods and Materials
A driven equilibrium diffusion prepared, multi-segmented Rotating Ultra-Fast Imaging Sequence (RUFIS)1 was developed, as shown in Figure 1. In the diffusion preparation, bipolar gradients and two pairs of pre-gradients are used to reduce eddy currents caused by large diffusion gradients. All the gradients are designed to use a sinusoidal shape to minimize the acoustic noise. Phase cycling is used in the tip-up 90° pulse (+X, +Y, -X and -Y) to compensate for T1 recovery during the RUFIS readout2, and also to correct eddy currents3.
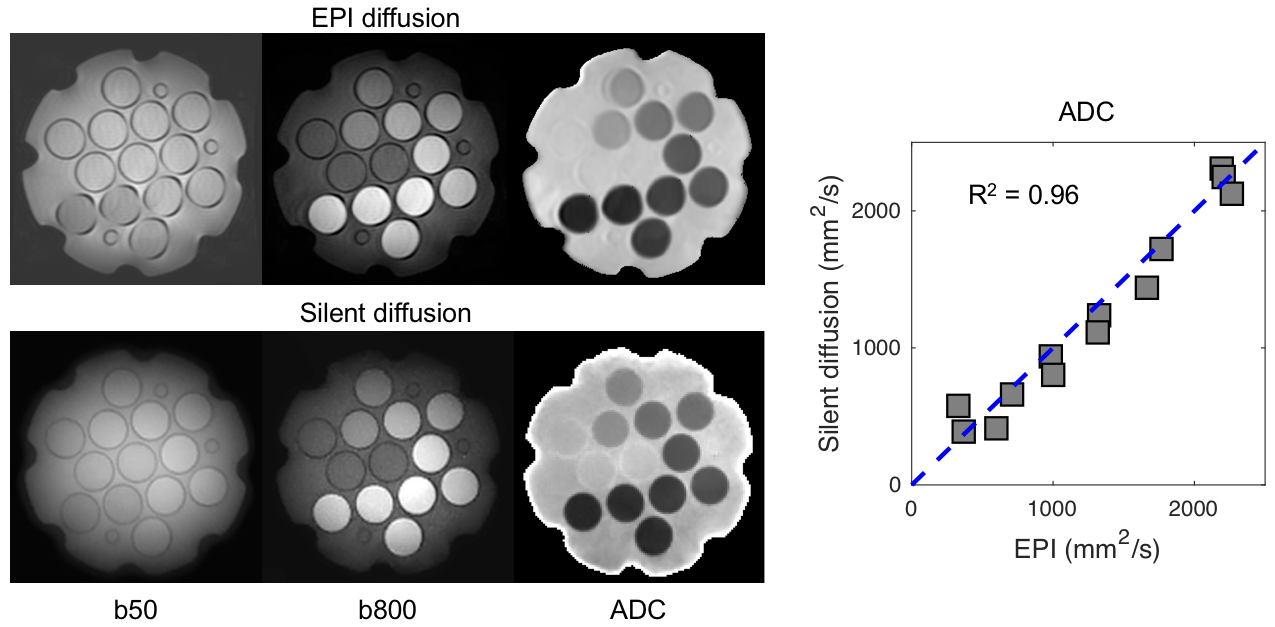
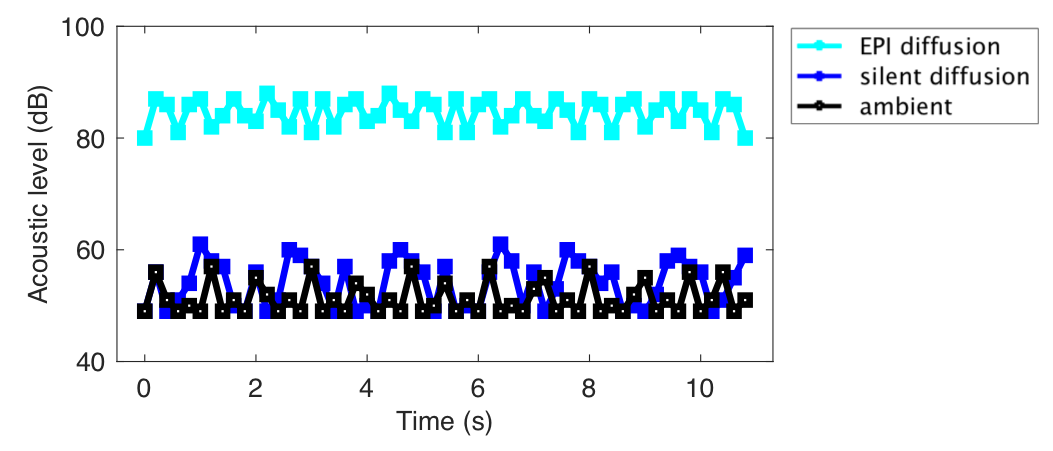
A diffusion phantom (Model 128, High Precision Devices) was used to validate the diffusion contrast and apparent diffusion coefficient (ADC) measurement of the sequence. A power monitor (RadioShack, Boston, MA) was placed three meters away from the scanner, directly pointing at the scanner bore, in order to measure the acoustic noise of the proposed silent DWI, conventional DW-EPI, and ambient noise in the MRI scan room.
With IRB approval and informed consent/assent, the sequence was validated in the prostate in five male volunteers and in the knee in six volunteers (three males). Image quality and prostate ADC values were compared with DW-EPI sequence using a paired t-test. Ten pediatric patients were scanned using the silent diffusion sequence. The images were compared with other routine sequences.
All scans were performed in a 3T scanner (MR750, GE Healthcare, Waukesha, WI). A 16 channel Flex coil was used for the knee and 32 channel body coil was used for the prostate scan. The in-vivo images were acquired using a 128×128 matrix size and a slice thickness of 4 mm. 384 views-per-segment were used. In the knee scans, the FOV was 16×16 cm2, b = 50, 400 s/mm², and the overall scan time was 6 mins. In the prostate scan, the FOV was 20×20 cm2, b = 50, 600 s/mm², and the scan time was 5 mins. The DW-EPI sequence used the same scan parameters, with a resulting scan time of 1 min for knee and 2 mins for prostate.
Results
In the phantom scans, the use of phase-cycled RF pulse corrected eddy currents from the diffusion gradients and eliminated the T1 recovery from the RUFIS acquisition. In high b-value images, the image contrast for both DW-EPI and silent diffusion was similar. The ADC measurement of the silent diffusion sequence correlates very well with that from the DW-EPI sequence (R2 = 0.96, Figure 2).
From the acoustic noise measurement, DW-EPI is much louder than silent DWI (85 ± 2.4 vs. 54 ± 2.4 dB), while latter approaches ambient noise (51 ± 2.8 dB), as shown in Figure 3.
In volunteer images, DW-EPI suffers from large image distortion near the tissue-air interface, such as the anterior part of the knee, and in the prostate peripheral zone near the rectum, while silent diffusion sequence provides distortion free images, as shown in Figure 4. The volunteer prostate ADC value in silent diffusion shows no significant difference with DW-EPI (1.4 ± 0.2 vs. 1.3 ± 0.1 ×10-3 mm2/s, p = 0.3).
In patient scans, the lesions are observed in the silent diffusion sequence, and are proved by conventional T2w sequence (Figure 5).
Discussion
The proposed silent diffusion sequence provides similar diffusion contrast with improved image quality compared to EPI diffusion in phantom and in-vivo scans. However, there are some limitations. First, it has a longer scan time compared to EPI diffusion. Second, the phase incoherence is not corrected between segments currently, which makes the sequence sensitive to motion and limits the use of high b-values. Future work should focus on solving these problems for a more wider application of the sequence.Conclusion
We have developed a silent and distortion-free diffusion imaging sequence that provides comparable diffusion contrast and ADC measurement with DW-EPI. This sequence could improve image quality and patient comfort for clinical MRI.Acknowledgements
We acknowledge support from GE Healthcare, P41 EB015891, NIH R01 EB009690 and NIH R01 HL136965.References
1. David Madio, Irving Lowe. Ultra-fast imaging using low flip angles and FIDs. Magn Reson Med. 1995 Oct;34(4):525-9.
2. Jean Coremans, Marc Spanoghe, Lubos Budinsky, et al. A comparison between different imaging strategies for diffusion measurements with the centric phase-encoded turboFLASH sequence. J Magn Reson. 1997 Feb;124(2):323-42.
3. David Thomas, Gaby Pell, Mark Lythgoe, et al. A quantitative method for fast diffusion imaging using magnetization-prepared TurboFLASH. Magn Reson Med. 1998 Jun;39(6):950-60.
Figures