3471
Diffusion kurtosis imaging–derived histogram metrics for prediction of KRAS/NRAS/BRAF mutations in rectal adenocarcinoma: Preliminary findingsYanfen Cui1, Zhizheng Zhuo2, and Xiaotang Yang1
1Shanxi Province Cancer Hospital, Taiyuan, China, 2MR Clinical Sciences, Philips Healthcare Greater China, Beijing, China
Synopsis
It was revealed that DKI metrics with whole-tumor volume histogram analysis, especially the K75th parameter, yielded more preferable AUC and specificity values for predicting KRAS/NRAS/BRAF mutations than ADC and D values, and thus may potentially serve as an optimal imaging biomarker for the prediction of KRAS/NRAS/BRAF mutations for guiding targeted therapy.
Purpose:
Several studies have shown that metastatic CRCs with RAS mutations tend to be resistant to therapies with antibodies targeted to the epidermal growth factor receptor (EGFR) [1, 2]. Panitumumab and cetuximab, anti-EGFR monoclonal antibodies, are currently recommended for only metastatic CRC patients with wild-type KRAS and NRAS [4]. Furthermore, BRAF and KRAS mutations are mutually exclusive and have the same tumorigenic effects [4]. Therefore, KRAS/NRAS/BRAF mutational test has been incorporated into routine clinical practice for guiding targeted therapy. However, imaging identification of KRAS/NRAS/BRAF mutations in CRC has received little attention. Therefore, the present study aimed to evaluate the potential role of DKI-derived parameters by using histogram analysis obtained from whole-tumor volumes for prediction of the status of KRAS/NRAS/BRAF mutations in patients with rectal adenocarcinoma.Methods:
This retrospective study was approved by our institutional review board and written informed consent was waived. 152 consecutive patients with rectal adenocarcinoma were retrospectively evaluated. All patient underwent MRI examination at 3.0 T scanner (Achieva; Philips Healthcare, Best, The Netherlands) with 8-channel phased array torso coils, including T2-weighted imaging (T2WI), diffusion kurtosis imaging (DKI) and contrast enhanced T1-weighted imaging. DKI was performed using a single-shot EPI sequence with multiple b-values (b = 0, 700, 1400, and 2100 s/mm2). Key acquisition parameters for DKI were as follows: TR/TE = 4,000/80 ms; flip angle= 90°; parallel imaging acceleration factor = 2; slice thickness = 3 mm, no slice gap; field of view (FOV) = 25 cm × 25 cm; matrix = 256 ×256; Total imaging time for DWI = 3 min 51 s. The relationship between signal variation and the multiple b-values is expressed as: Sb/S0=exp(-b·D + b2·D2·K/6), where Sb is the DWI signal intensity at a specific b value, S0 is the baseline signal intensity without diffusion gradient, D is a corrected ADC related to Gaussian behavior, and K is a dimensionless parameter signifying the kurtosis coefficient. The ADC map was generated from the same dataset using a standard mono-exponential model Sb/S0= exp (–b ·ADC). All image processing and analysis were performed using customized software developed in Matlab (Mathworks Inc, MA). For each patient, Regions of interests (ROIs) were manually drew on each consecutive DWI maps with b= 1400 or 2100 sec/mm2 along the border of the tumor, covering the whole lesion while excluding the cystic, necrosis and hemorrhage areas by referring to the conventional MR images, by one experienced radiologists who were both blinded to all the clinical information. The quantitative parameters of D, K, and conventional apparent diffusion coefficient (ADC) were measured using whole-tumor volume histogram analysis. Student’s t-test or Mann-Whitney U-test, receiver operating characteristic(ROC) curves were used for statistical analysis. All statistical analyses were performed using SPSS 19.0(IBM, New York, NY, USA) and MedCalc 15.8 (MedCalc,Mariakerke, Belgium).Results:
All the percentiles metrics of ADC and D values were significantly lower in the mutated group than those in the wild-type group (all P< 0.05), except for the minimum value of ADC and D (both P > 0.05), while K-related percentiles metrics were higher in the mutated group compared with those in the wild-type group (all P< 0.05). Regarding the comparison of the diagnostic performance of all the histogram metrics, K75th showed the highest AUC value of 0.866, and the corresponding values for sensitivity, specificity, PPV, and NPV were 67.57% and 92.31%, 89.29%, and 75.0%, respectively.Discussion and Conclusion:
The findings of our study suggested that the majority of the DKI-derived histogram metrics can be used to distinguish KRAS/NRAS/BRAF mutations from wild-type ones in patients with rectal cancer. More interestingly, K-related percentiles metrics, especially K75th, yielded more preferable AUC and specificity for predicting KRAS/NRAS/BRAF mutations than ADC and D values. However, the baseline clinical and histopathological characteristics were not associated with KRAS/NRAS/BRAF mutations. Therefore, DKI-derived histogram metrics, especially K, may potentially serve as an optimal imaging biomarker for the prediction of KRAS/NRAS/BRAF mutations for guiding targeted therapy.Acknowledgements
This study was supported by the Science and Technology Project of Shanxi Province (Grant No. 20150313007-5).References
- Peeters M, Oliner KS, Price TJ, et al (2015) Analysis of KRAS/NRAS Mutations in a Phase III Study of Panitumumab with FOLFIRI Compared with FOLFIRI Alone as Second-line Treatment for Metastatic Colorectal Cancer. Clin Cancer Res 21:5469-5479.
- Bokemeyer C, Kohne CH, Ciardiello F, et al (2015) FOLFOX4 plus cetuximab treatment and RAS mutations in colorectal cancer. Eur J Cancer 51:1243-1252.
- Allegra CJ, Rumble RB, Hamilton SR, et al (2016) Extended RAS Gene Mutation Testing in Metastatic Colorectal Carcinoma to Predict Response to Anti-Epidermal Growth Factor Receptor Monoclonal Antibody Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update 2015. J Clin Oncol 34:179-185.
- Rajagopalan H, Bardelli A, Lengauer C, et al (2002) Tumorigenesis: RAF/RAS oncogenes and mismatch-repair status. Nature 418:934.
Figures
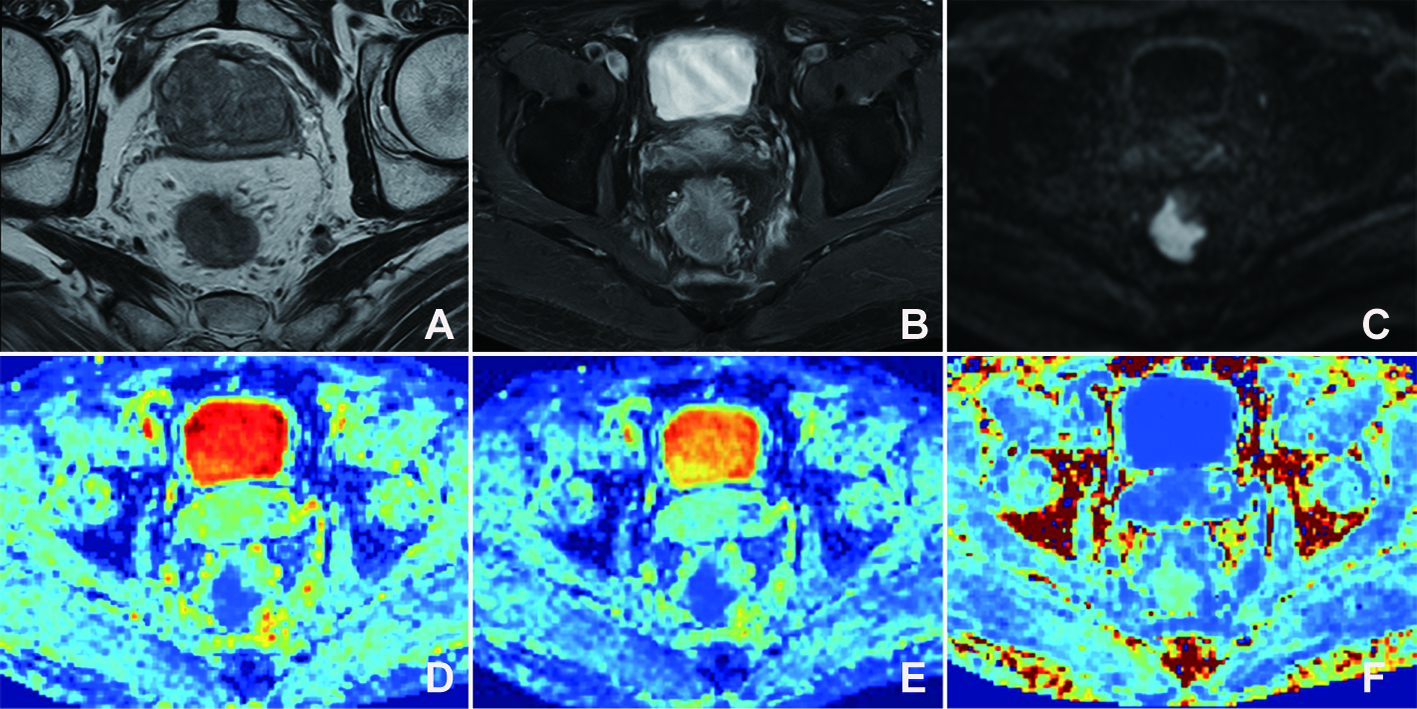
Figure 1. MR images of a 46-year-old man
with mutated KRAS. Axial T2-weighted MR (A) and contrast T1-weighted MR image
(B) show a mass occupying more than three-quarters of the rectal wall, with
mild enhancement. (C) High-b-value (1400 s/mm2) DW image shows hyperintense
tumor. The color-coded ADC map (D),D map (E) and K map (F) show heterogeneous
blue color in the corresponding tumor with ADCmean of 0.903 × 10-3 s/mm2, Dmean
of 1.087 × 10-3 s/mm2, and Kmean value of 1.08.
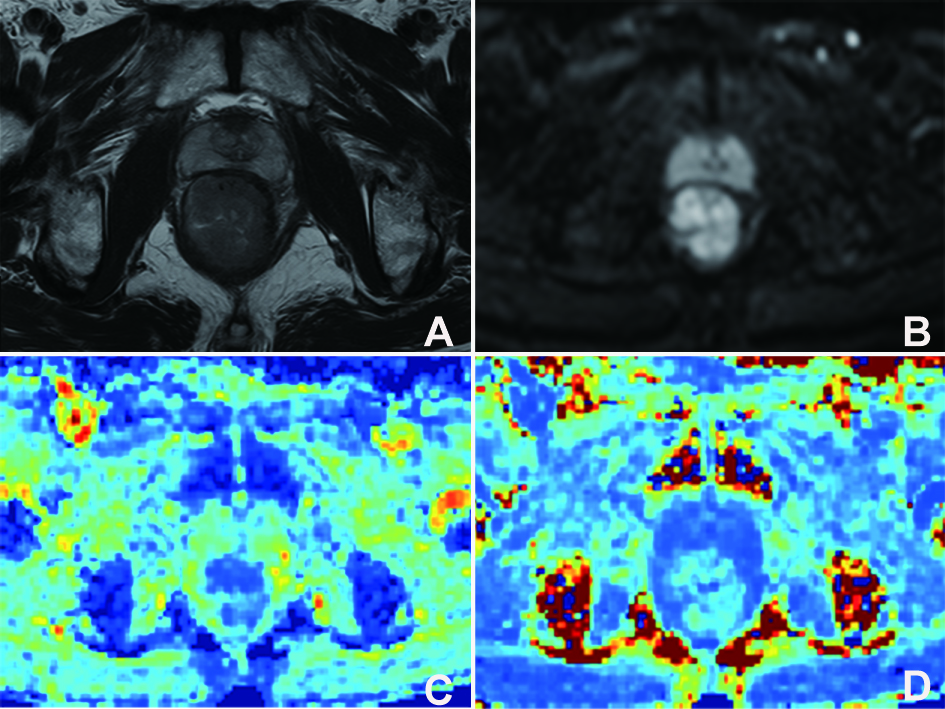
Figure 2. MR images of a 61-year-old woman
with wild-type KRAS/NRAS/BRAF. Axial T2-weighted MR image (A) shows a mass
occupying more than three-quarters of the rectal wall. (B) High-b-value (1400
s/mm2) DW image shows hyperintense tumor. The color-coded D map (C) and K map
(D) show heterogeneous blue color in the corresponding tumor with
Dmean of 1.164 × 10-3 s/mm2 and Kmean value of 0.913.
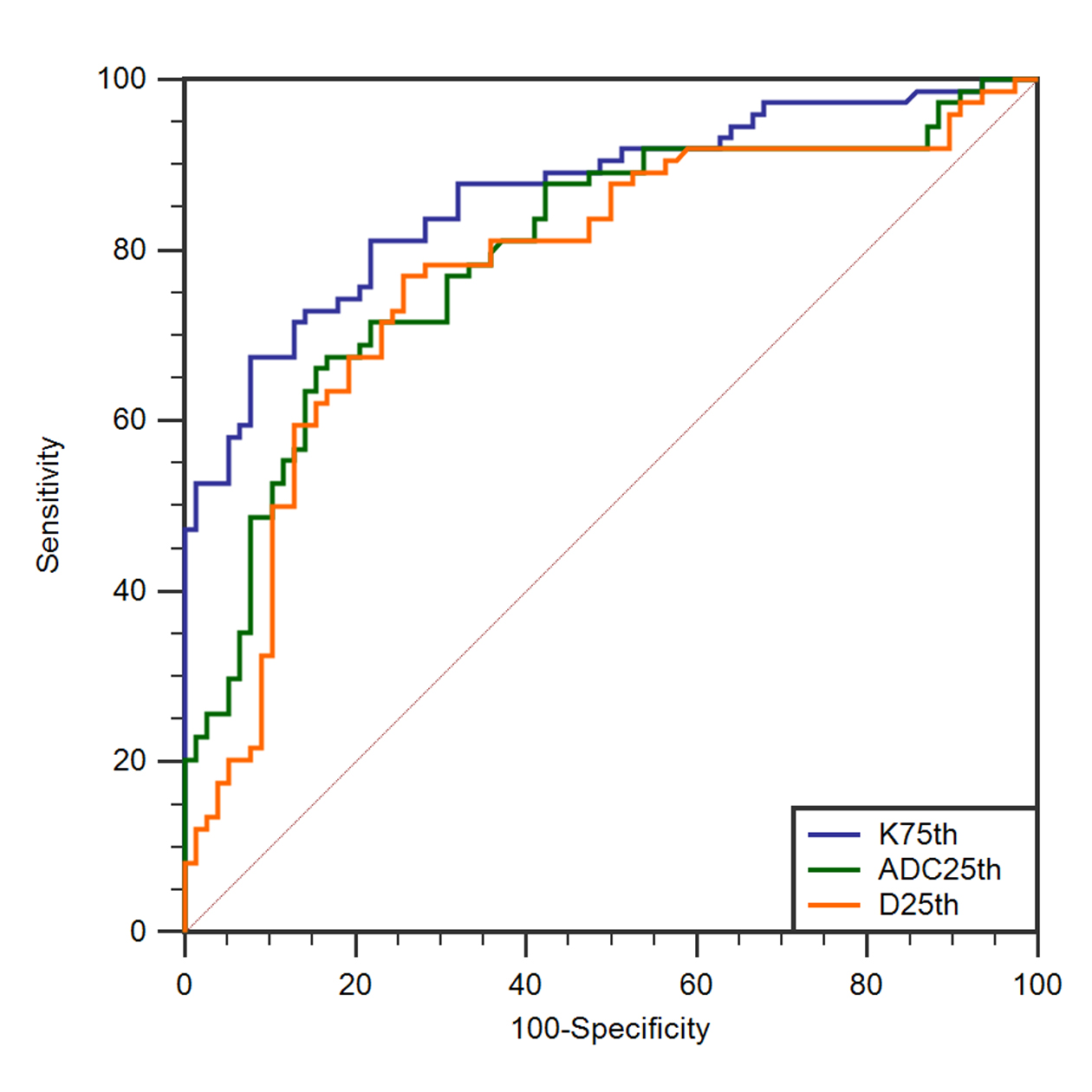
Figure 3. Comparing the diagnostic ability
for discriminating KRAS/NRAS/BRAF mutations between histogram values of ADC25th,
D25th, and K75th. ROC analysis shows that the K75th had the higher AUC value (0.866)
than that of the others. When the cutoff value for K75th was 1.070, the
corresponding values for sensitivity, specificity, PPV and NPV were 67.57%, 92.31%,
89.29%, and 75.01%, respectively.