3456
A Comparative Study of IVIM Model, Kurtosis Model and IVIM-Kurtosis Model for the Diagnosis and Aggressiveness Assessment of Prostate Cancer1Beijing Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
The purpose of our study
was to
quantitatively compare the utility of the parameters obtained from IVIM, kurtosis, and
IVIM-kurtosis models in the differential diagnosis and aggressiveness
assessment of prostate cancer, by using in-bore transrectal MR-guided biopsy as
a reference. Our results displayed that IVIM, kurtosis and IVIM-kurtosis models
has effective function for the differential diagnosis of prostate cancer and
the diagnostic efficacy among the three models were similar.
In aggressiveness assessment, IVIM-kurtosis model
may be superior to the others.
Introduction
Methods
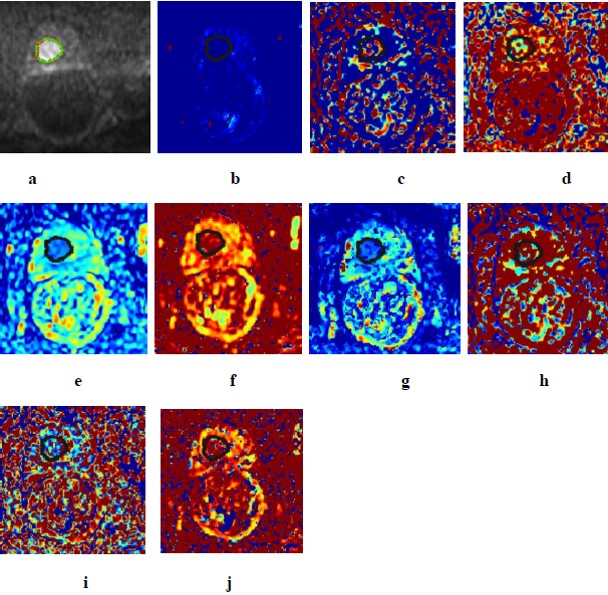
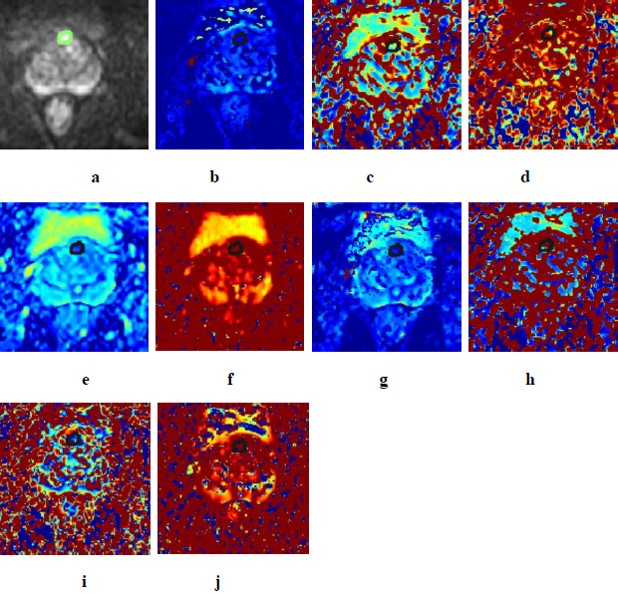
Thirty patients were recruited in this study. Diffusion-Weighted Images were acquired on a 3.0T MR scanner with an eight-channel cardiac coil using 0 b values up to 2000s/mm2 and analyzed using three models, including IVIM model (diffusion coefficient(DIVIM), pseudo diffusion coefficient (D*IVIM), perfusion fraction (fIVIM)), kurtosis model (diffusion coefficient(Dkurtosis), kurtosis(Kkurtosis) and IVIM-kurtosis model(diffusion coefficient(DIVIM-kurtosis), pseudo diffusion coefficient (D*IVIM-kurtosis), perfusion fraction(fIVIM-kurtosis), kurtosis (KIVIM-kurtosis)). All patients were histologically confirmed by subsequently in-bore MR-guided biopsy, including 13 prostate cancer and 17 BPH and /or prostatitis. The values of these parameters were calculated and compared between cancerous and non-cancerous groups. Diagnosis performances of all parameters and models were evaluated by receiver operating characteristic (ROC) analysis. Correlations of these parameters and Gleason scores of prostate cancer were evaluated by Pearson test.Results
(1) DIVIM, fIVIM, Dkurtosis and DIVIM-kurtosis value were significantly lower in prostate cancer than those of prostatitis and benign prostatic hyperplasia (P=0.010, P=0.003, P<0.001, P=0.001). Kkurtosis and KIVIM-kurtosis value were significantly higher in prostate cancer than those of prostatitis and benign prostatic hyperplasia(P=0.038, P=0.042). D*IVIM-kurtosis value was significantly lower in prostate cancer than those of prostatitis (P=0.035). (2) The AUC of Dkurtosis and DIVIM-kurtosis showed higher value than D*IVIM-kurtosis, with statistical significance, and no statistically significant differences were observed between other parameters. The AUC of IVIM model, kurtosis model and IVIM-kurtosis model showed no significant differences. (3) fIVIM-kurtosis and KIVIM-kurtosis values correlated positively with Gleason scores (r=0.665, P=0.013; r=0.689, P=0.019). D*IVIM-kurtosis value correlated negatively with Gleason scores (r=-0.589, P=0.034).Discussion
In this study, our results showed DIVIM, Dkurtosis, fIVIM, DIVIM-kurtosis, Kkurtosis and KIVIM-kurtosis can provide information to differentiate prostate cancer from prostatitis/BPH. D*IVIM-kurtosis value was significantly lower in prostate cancer than those of prostatitis, while D*IVIM and fIVIM-kurtosis of PCa was indistinguishable from noncancerous foci. The results of D* and f among previous studies were various5,6,7, the contributing factors may be D* and f were susceptible to measurement and noise variations. Our study revealed that the diagnostic accuracies of IVIM, kurtosis and IVIM-kurtosis seemed to be similar. Li et al found that the AUC of IVIM and DKI showed no statistical difference8, which was in accordance with our study. In aggressiveness assessment, we observed that fIVIM-kurtosis and KIVIM-kurtosis positively correlated with Gleason scores, while D*IVIM-kurtosis negatively correlated with Gleason scores. But the parameters derived from IVIM and kurtosis models had no significant correlations with Gleason scores. The results indicated that IVIM-kurtosis can provided more information in grading of PCa compared with IVIM and kurtosis models. A limitation of our study is the patient population was relatively small. Further studies with larger samples may be needed to observe the clinical benefit of the three models.Conclusion
IVIM model, Kurtosis model and IVIM-Kurtosis model are all useful for the diagnosis of prostate cancer and the diagnostic efficacy seemed to be similar for these three models. In the other hand, the IVIM-kurtosis model may be superior to IVIM model and kurtosis model for the aggressiveness assessment of prostate cancer.Acknowledgements
No acknowledgement found.References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018.
2. Wang X, Tu N, Qin T, et al. Diffusion Kurtosis Imaging Combined With DWI at 3-T MRI for Detection and Assessment of Aggressiveness of Prostate Cancer. AJR Am J Roentgenol. 2018;211(4):797-804.
3. Pesapane F, Patella F, Fumarola E M, et al. Intravoxel Incoherent Motion (IVIM) Diffusion Weighted Imaging (DWI) in the Periferic Prostate Cancer Detection and Stratification. Medical Oncology. 2017;34(3):35.
4. Si Y, Liu RB. Diagnostic Performance of Monoexponential DWI Versus Diffusion Kurtosis Imaging in Prostate Cancer: A Systematic Review and Meta-Analysis. AJR Am J Roentgenol. 2018;211(2):358-368. 5. Valerio M, Zini C, Fierro D, et al. 3T multiparametric MRI of the prostate: Does intravoxel incoherent motion diffusion imaging have a role in the detection and stratification of prostate cancer in the peripheral zone? European Journal of Radiology. 2016;85(4):790-794.
6. Kuru TH, Roethke MC, Stieltjes B, et al. Intravoxel incoherent motion (IVIM) diffusion imaging in prostate cancer - what does it add? Journal of computer assisted tomography. 2014;38(4):558-564.
7. Döpfert J, Lemke A, Weidner A, Schad LR. Investigation of prostate cancer using diffusion-weighted intravoxel incoherent motion imaging. Magnetic Resonance Imaging. 2011;29(8):1053-1058.
8. Li
C, Chen M, Wan B, et al. A comparative study of Gaussian and non-Gaussian
diffusion models for differential diagnosis of prostate cancer with in-bore
transrectal MR-guided biopsy as a pathological reference. Acta Radiologica. 2018;
59(11):1395-1402.
Figures