3453
Head and neck squamous cell carcinoma: diagnostic performance of diffusion kurtosis imaging for the prediction of histopathologic prognostic factors1Radiology, Peking Union Medical College Hospital, Beijing, China, 2Pathology, Peking Union Medical College Hospital, Beijing, China, 3Otolaryngology, Peking Union Medical College Hospital, Beijing, China, 4Stomatology, Peking Union Medical College Hospital, Beijing, China, 5Siemens Healthcare Ltd., Beijing, China, 6Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
This preliminary study evaluated the diagnostic efficacy of diffusion parameters, derived from different models, for differentiating between tumor grades and identifying metastatic lymph nodes in head and neck squamous cell carcinomas (HNSCCs). Superior diagnostic efficiency was achieved when combining ADC values derived from a mono-exponential model with kurtosis and diffusivity values derived from a diffusion kurtosis imaging (DKI) model compared to using each parameter by itself.
Introduction
Lymph node involvement and poor differentiation of tumor cells have long been indicated as the most important factors in determining the prognosis of head and neck squamous cell carcinoma (HNSCC). In this preliminary study, we aimed to evaluate the diagnostic efficiency of diffusion kurtosis imaging (DKI)–derived parameters as well as ADC values derived from a mono-exponential model, for determining tumor grade and lymph node status in HNSCCs.Methods
HNSCC patients who underwent tumor resection and bilateral lymphadenectomy were included in our study. MR data were collected on a MAGNETOM Skyra 3T MR scanner (Siemens Healthcare, Erlangen, Germany) with a 20-channel head-neck coil and a pair of 4-channel special-purpose coils. Diffusion-weighted images were acquired using a prototype readout-segmented echo-planar imaging (RESOLVE) pulse sequence with simultaneous multi-slice (SMS) and the following parameters: TR/TE = 4080/66 ms, slice thickness = 3 mm; voxel size = 1.5 × 1.5 × 3.0 mm3; FOV = 160 × 160 mm2; readout segments = 5; slice acceleration factor = 2; b value = 0, 800 and 1600 s/mm2; bandwidth = 689 Hz/pixel; and total acquisition time = 4:47 mins. The ADC values were calculated using the mono-exponential model below either with two b values of 0, 800 s/mm2 (ADC2b) or with three b values (ADC3b):$S(b)=S0exp(-ADC·b)$.The DKI parameters of kurtosis and diffusivity were fitted according to:$S(b)=S0exp(-b·D+1/6b2·D2·K)$.
where b is the diffusion-weighting factor, and S (b) and S0 are the signal intensities with and without diffusion-sensitizing gradients, respectively. All parameter maps were generated using the prototype Body Diffusion Toolbox software (Siemens Healthcare, Erlangen, Germany). The regions of interest (ROIs) were drawn manually on the corresponding maps on a single slice in which the size of the tumor or lymph node was the largest. The tumors were histopathologically classified into well and moderately-to-poorly differentiated carcinoma groups. The patients were then divided into two groups according to the presence or absence of lymph node metastases. Student's t-tests and receiver operating characteristic curves were used. A p value of ≤0.05 was considered statistically significant.
Results
Data from 43 patients (35 males; median age, 59.6 years; age range, 31–85 years) with HNSCCs (19 oral cavity carcinoma, 20 hypopharyngeal carcinomas, 2 oropharyngeal carcinomas, and 2 laryngeal carcinomas) were collected and analyzed. Cervical lymph node involvement was identified in 12 patients. The tumors were histopathologically classified into 11 well differentiated, 12 well-moderately differentiated, and 21 moderately-to-poorly differentiated tumors.
Between the 11 well differentiated and 21 moderately-to-poorly differentiated tumors, there were no significant differences between ADC2b values, ADC3b values, and kurtosis and diffusivity (as shown in Table 1) values. The areas under the ROC curve for the four parameters (as shown in Table 2) showed poor diagnostic efficiency of each parameter alone for histologic differentiation of HNSCCs. When two or more parameters were combined, the areas under the ROC curve were higher. Optimal diagnostic efficacy was derived when combining ADC2b with kurtosis and diffusivity, with an AUC of 0.753, a sensitivity of 71.43%, and a specificity of 81.82%.
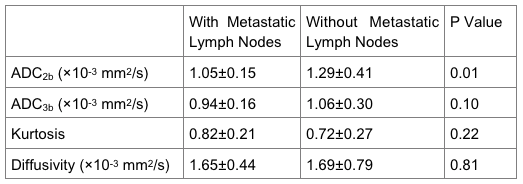
ADC2b values were significantly lower in tumors of patients with metastatic lymph nodes than those without (p value= 0.01). The areas under the ROC curve (as shown in Table 4) showed relatively good efficacy of ADC2b values of tumors for determining lymph nodes status. Optimal diagnostic efficiency was derived when combining ADC2b with kurtosis and diffusivity, with an AUC of 0.738, a sensitivity of 91.67%, and a specificity of 53.57%. Other parameters derived from DKI showed no significant differences between the two groups (as shown in Table 3).
Parameters were calculated in 39 benign lymph nodes and 29 metastatic lymph nodes. Between the metastatic and benign lymph nodes, there were no significant differences of the four parameters. The areas under the ROC curve showed limited diagnostic efficiency for differentiating between metastatic and benign lymph nodes, with the highest AUC being 0.632.
Discussion and Conclusion
DKI has been recently proposed to provide more description of diffusion processes and reflect heterogeneous pathology of tumor. Several papers demonstrated the high diagnostic value of these imaging modalities in differentiating between benign and malignant tumors, in determining tumor histological grades in brain and head and neck region. However, the kurtosis and diffusivity values of primary lesions by themselves in our study showed limited diagnostic efficiency for indicating histologic differentiation grades and for identifying metastatic lymph nodes, possibly due to the limited sample size and several locations of primary tumors.
In our study, the combined ADC values and DKI parameters showed more promise for preoperative assessment of histologic grade and presence of lymph node metastasis. Further research on the use of this combination of parameters should be conducted and validated in a study with a larger sample.
Acknowledgements
No acknowledgement found.References
No reference found.Figures