3452
The performance of TGSE BLADE DWI in the diagnosis of cholesteatoma compared with RESOLVE DWI technique1EENT Hospital of Fudan University, Shanghai, China, 22.Scientific Marketing, Siemens Healthcare, Shanghai, China, 3Department of Digitalization, Siemens Shenzhen Magnetic Resonance Ltd, Shenzhen, China, 4Scientific Marketing, Siemens Healthcare, Shanghai, China
Synopsis
Synopsis:This study aimed to compare the performance of two diffusion weighted imaging techniques used to diagnose cholesteatoma: readout-segmented echo-planar imaging (RESOLVE) and turbo gradient spin echo (TGSE) BLADE DWI. The results showed that the TGSE BLADE DWI had better image quality with respect to reducing susceptibility artifacts, distortion, and blurring compared with RESOLVE. However, the SNR of TGSE BLADE DWI needs to be improved in the future.
Introduction
Cholesteatoma is a benign, gradually expanding and destructive epithelial lesion of the temporal bone which results in the erosion of adjacent bony structures and may lead to various complications.1 High-resolution CT remains the primary imaging technique for the diagnosis and characterization of the middle ear cholesteatoma, but it is difficult to distinguish cholesteatoma on imaging from granulation tissue, fibrous tissue, or fluid2. Many studies have shown that MR diffusion weighted imaging (DWI) has a high sensitivity and specificity for identifying the presence of cholesteatoma due to its high keratin content. However, as conventional DWI uses an echo planar imaging (EPI) trajectory to collect k-space data, the obtained images may suffer from sever susceptibility artifacts at air-bone interfaces. Additionally, the image resolution is limited. Thus, it is difficult to perform DWI for a lesion less than 5 mm3,4 close to the distortion area. In order to reduce the image distortion, readout-segmented echo-planar imaging (RESOLVE) has been proposed, and can significantly improve head and neck DW images by reducing the echo spacing. However, BLADE DWI technique has been reported to be able to eliminate susceptibility artifacts by applying the ‘blades’ acquisition scheme in k-space5. Such a non-EPI technique was further optimized by using a turbo gradient spin echo method to increase the SNR efficiency, so that it can achieve the detection of small-sized cholesteatomas (>2mm) and to increase resolution to decrease susceptibility artifacts allowing for differentiation from granulation tissue5. The purpose of this study aimed to evaluate the role of the TGSE BLADE DWI technique in the diagnosis of cholesteatoma and to qualitatively and quantitatively compare the image qualities between TGSE BLADE method and RESOLVE.Methods
A total of 22 patients (14 males and 8 females; age range 10–56 years; mean 35.5 years) with surgically confirmed cholesteatoma were enrolled in this study from October 2018 to November 2018. All of them underwent DWI (both the prototype TGSE BLADE DWI sequence and the commercially available RESOLVE DWI) using a 3T scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a 64-channel brain coil. The parameters for TGSE BLADE DWI were as follows: TR/ TE = 4000/62 ms, slice thickness/gap = 2/0.2 mm, slices = 21, bandwidth = 520 Hz/Px, field of view (FOV) = 280 × 280 mm2, matrix = 192 × 192, voxel size = 1.5 × 1.5 × 2.0 mm3, number of excitations (NEX) = 1, diffusion directions = 4, b = 0, 1000 s/mm2, turbo factor = 13, EPI factor = 3, and the data acquisition time was 3min46s. For REOSLVE DWI, the imaging parameters were: TR/TE = 5020/53 ms, slice thickness/gap = 2/0.2 mm, slices = 21, bandwidth =766Hz/Px, field of view (FOV) = 230 × 230 mm, matrix = 192 × 192, voxel size = 1.2 × 1.2 × 2.0 mm, diffusion directions = 4, b = 0, 1000 s/mm2, and the data acquisition time was also 3min46s. Qualitative imaging parameters (imaging sharpness, geometric distortion, ghosting artifacts, and overall imaging quality) and quantitative imaging parameters (ADC, SNR, contrast, and contrast-to-noise ratio (CNR)) for the two diffusion acquisition techniques were assessed by two independent radiologists. Results
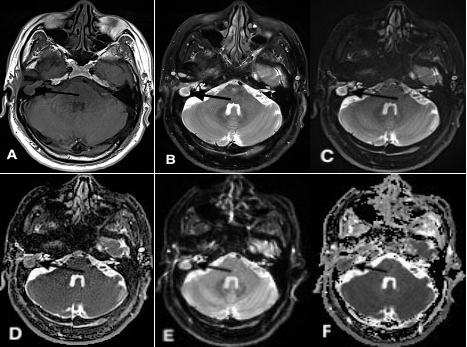
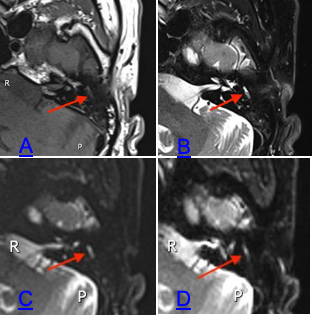
The comparisons of the qualitative scores indicated that TGSE BLADE DWI produces less geometric distortion and ghosting artifacts (P<0.001), a sharper image (P<0.05), and higher image quality (P<0.001) than RESOLVE DWI. Furthermore, as shown in Figure 2, the Axial TGSE BLADE DWI image completely and clearly shows a small-lesion (1.7mm width) located in the left tympanic cavity and produces less geometric distortion than the RESOLVE DWI image. As shown in Figure 1, the TGSE DWI axial image precisely defines the cholesteatoma lesion in the right middle ear without geometric distortion and ghosting artifacts, whereas the RESOLVE DWI has significant artifacts at the air-bone interface (mastoid-the location of cholesteatoma lesion and nasal sinus). The ADC (P<0.001) measured by TGSE BLADE DWI is significantly lower than that measured by RESOLVE DWI. Meanwhile, TGSE BLADE DWI produced significantly lower SNR (P < 0.001) and higher parameters (both contrast and CNR (P < 0.001)) than that of RESOLVE DWI.
Discussion and Conclusion
Compared to RESOLVE DWI, TGSE BLADE DWI can significantly improve the image quality of cholesteatoma by reducing susceptibility artifacts, distortion and blurring. Moreover, TGSE BLADE DWI is more valuable for the diagnosis of small-sized (1-2mm) cholesteatomas. However, TGSE BLADE DWI is not without its disadvantages. The overall image SNR is slightly lower. Therefore the anatomical details of the air-bone interface are not well shown.Acknowledgements
No acknowledgement found.References
1.Louw L. Acquired cholesteatoma pathogenesis: stepwise explanations. The Journal of laryngology and otology. Jun 2010;124(6):587-593.
2.Yates PD, Flood LM, Banerjee A, Clifford K. CT scanning of middle ear cholesteatoma: what does the surgeon want to know? The British journal of radiology. Oct 2002;75(898):847-852.
3.Vercruysse JP, De Foer B, Pouillon M, Somers T, Casselman J, Offeciers E. The value of diffusion-weighted MR imaging in the diagnosis of primary acquired and residual cholesteatoma: a surgical verified study of 100 patients. European radiology. Jul 2006;16(7):1461-1467.
4. De Foer B, Vercruysse JP, Pilet B, et al. Single-shot, turbo spin-echo, diffusion-weighted imaging versus spin-echo-planar, diffusion-weighted imaging in the detection of acquired middle ear cholesteatoma. AJNR. American journal of neuroradiology. Aug 2006;27(7):1480-1482.
5.Dhepnorrarat RC, Wood B, Rajan GP. Postoperative non-echo-planar diffusion-weighted magnetic resonance imaging changes after cholesteatoma surgery: implications for cholesteatoma screening. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. Jan 2009;30(1):54-58.
Figures