3444
Non-Gaussian IVIM-DWI for prediction of locoregional failure in nasopharyngeal carcinoma1Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Radiation Oncology, Dana-Farber/Brigham and Women’s Cancer Center, South Weymouth, MA, United States, 3Radiation Oncology, Memoral Sloan Kettering Cancer Center, New York, NY, United States, 4Radiation Oncology Eye, Ear, Nose & Throat, Hospital of Fudan University, Shanghai, China, 5Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
The study aims to assess quantitative metrics derived from pretreatment NG-IVIM using multiple b-value diffusion weighted imaging data for predicting tumor with and without locoregional failure (LRF) in NPC patients. Kaplan-Meier method and the log-rank test were used to analyze differences between NPC patients with and without locoregional curves. Kaplan Meier results showed that the pre-treatment mean ADC and D value could predict LRF in NPC patients. The pretreatment NG-IVIM diffusion-weighted imaging will provide useful information for the selection of patients appropriate for definitive radiotherapy.
Introduction
Nasopharyngeal carcinoma (NPC) has been linked to Epstein-Barr virus (EBV)1. Studies have shown an advantage to concurrent chemoradiation in the treatment of advanced NPC2. Predicting early response to chemoradiation therapy has remarkable clinical benefit for patients with NPC, which can be used to optimize adaptive and personalized radiotherapy3. Diffusion-weighted imaging (DWI), which characterizes the Brownian motion of water molecules in tissue4, has shown promise in management of NPC 5. The cell membrane and organelle in tumor tissue deviates the Gaussian diffusion towards non-Gaussian (NG) 6. The multiple b-value dataset fitted with the extended intravoxel incoherent motion (IVIM) model accounts for the non-Gaussian behavior of water diffusion, which is denoted by K, (kurtosis coefficient)7,8. The K is regarded as an index of tissue microstructural complexity 6,9. The aim of this study was early diagnostic prediction of pretreatment quantitative imaging metric derived from the NG-IVIM model using multiple b-value DWI data in NPC patients.Methods
Patient: Our institutional review board approved this retrospective study and written informed consent was obtained from all eligible NPC patients prior to the pre-treatment (pre-TX) MRI study. Between November June 2014 and September 2016, a total of 28 NPC patients (median age: 43 years, range: 21-67 years; 19 M/9 F) were enrolled into the study, who were treated with chemoradiation therapy (dose 70Gy). ). The clinical response was based on standard-of-care imaging and clinical follow up after treatment completion up to 33 months. Treating Physician categorized the patients into 2 groups with and without locoregional failure (LRF).
DWI data acquisition: MRI protocol consisted of multi-planar T1/T2 weighted imaging followed by multiple b-value DWI on a 3.0T scanner (Ingenia, Philips Healthcare, Netherlands) using a neurovascular phased-array coil10. The multiple b-value DW-MRI images were acquired using a single shot spin echo planar imaging (SS-SE-EPI) sequence with TR/TE=4000/80 (minimum) ms, field of view (FOV)=20-24 cm, matrix=128×128, slices=8-10, slice thickness=5mm, number of excitation (NEX)=2 and b=0,20,50,80,200,300,500,800,1500,2000 s/mm2.
DWI data analysis: Multiple b- value DW data were fitted to (a) mono-exponential model, which calculates the apparent diffusion coefficient (ADC), and (b) bi-exponential model (NG-IVIM), which provides estimate of the true diffusion coefficient (D), perfusion fraction (f), pseudo diffusion coefficient (D*), and kurtosis coefficient (K) 7,8. Regions of interest (ROIs) were delineated on the primary tumor by radiation oncologists on the multiple b- value DW image (b = 0 s/mm2) using ImageJ software11. All DW data analysis was performed using in-house software MRI-QAMPER (Quantitative Analysis Multi-Parametric Evaluation Routines) written in MATLAB (MathWorks, Natick, MA). ROI analyses, which yielded mean and standard deviation, were reported for the results.
Statistical analysis: The logistic regression was conducted on each variable against locoregional failure (LRF). The receiver-operating characteristic (ROC) curves were used to select the optimal cut-off point for quantitative metrics (i.e., ADC, D, D*, K and f) by maximizing the Youden index. Kaplan-Meier analysis was conducted on the two groups obtained by dichotomizing each variable based on the cut-off point; the difference in two curves was assessed using log-rank test. A p value <0.05 was considered statistically significant. Statistical computations were performed using R (R Core Team, Vienna, Austria)12.
Results
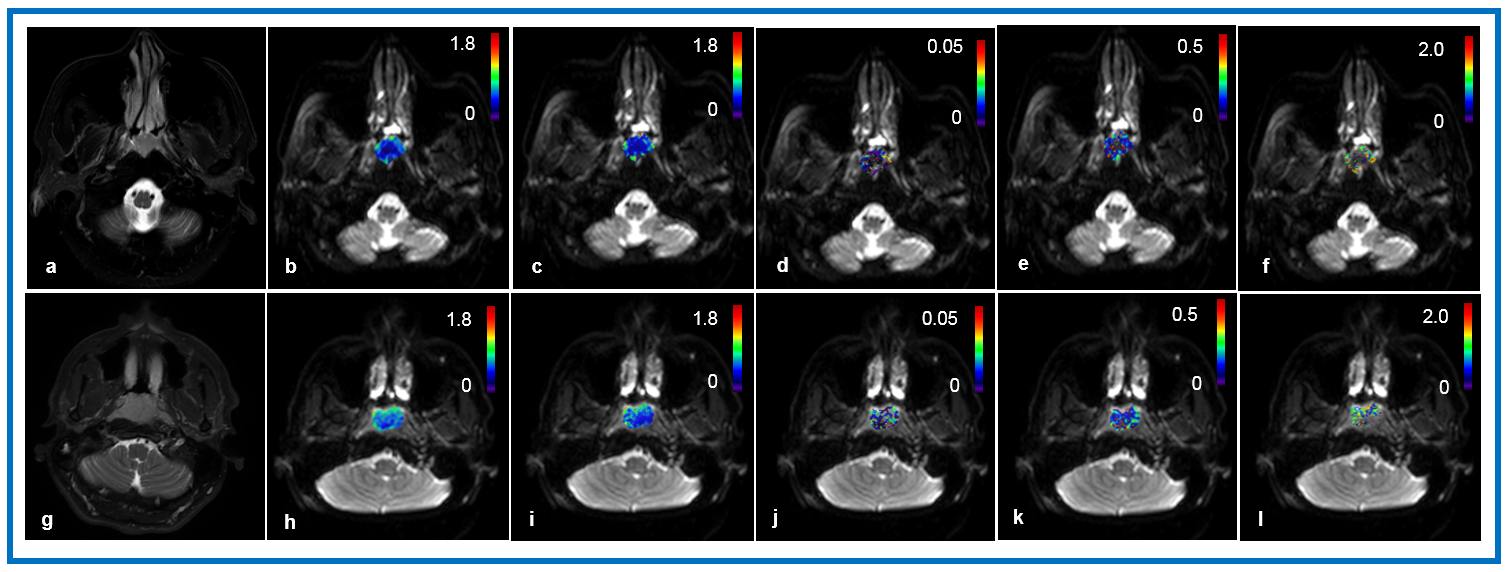
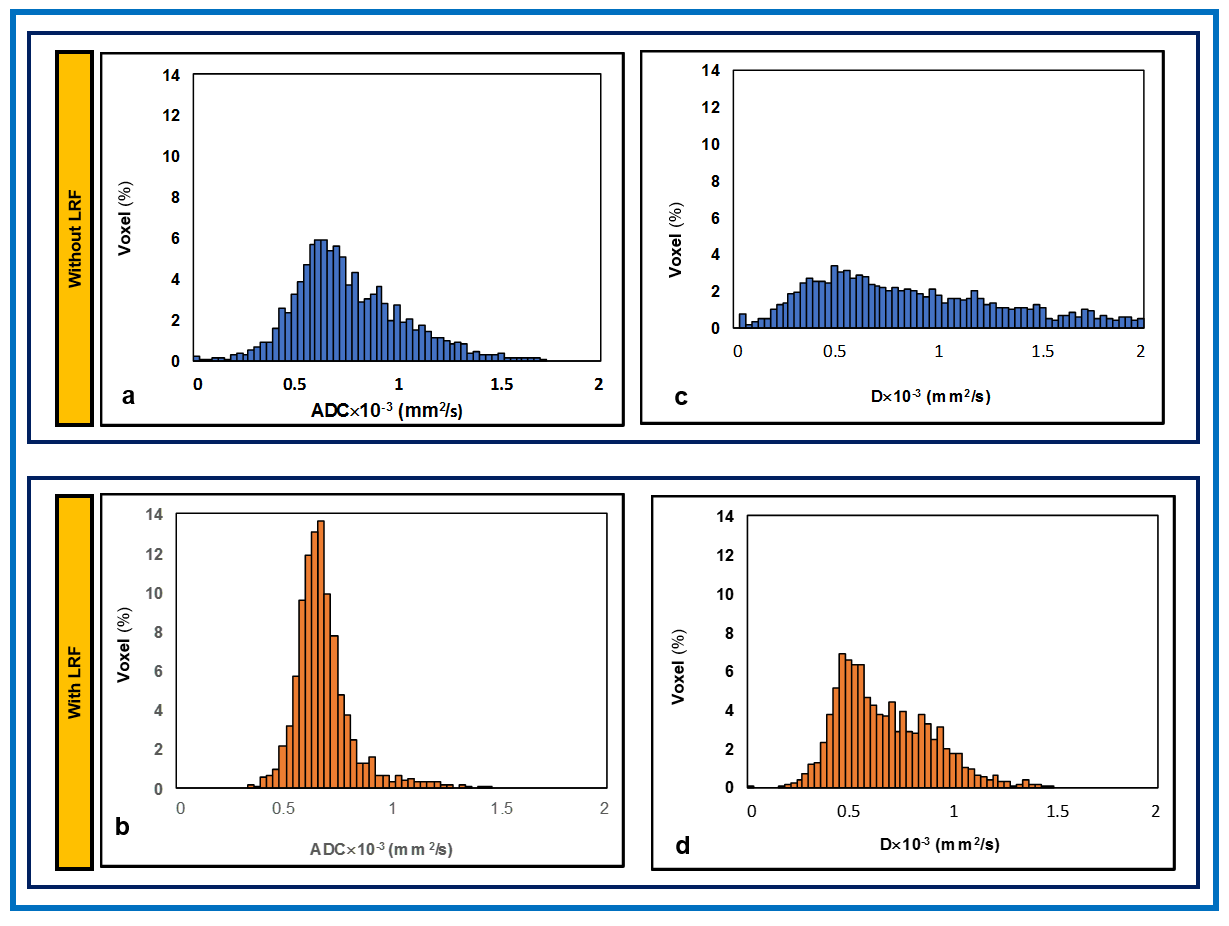
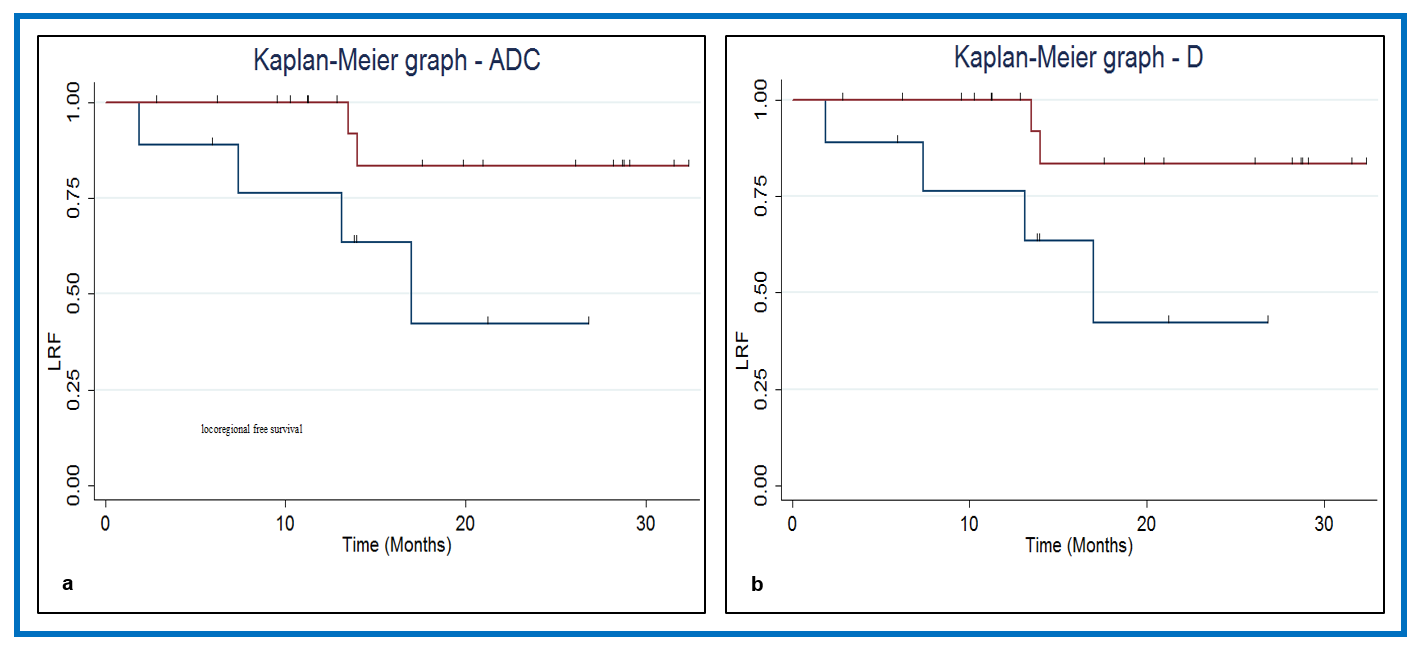
Figure 1 illustrates T2w MR images and primary tumor parametric maps of ADC, D, D*, f and K overlaid on DW image (b=0 s/mm2) from two NPC patients without LRF (46 years, male) and with LRF (43 years, female). NPC patients with and without LRF showed moderate change in metric values by 13%, 15%, 4%, 15% and 7% for ADC, D, D*, K, and f respectively. Figure 2 exhibits the histogram distributions of ADC and D of tumors with and without LRF in NPC patients. Figures 3 (a) and (b) display the Kaplan Meier plots for ADC and D with p = 0.034 and p = 0.045, respectively with optimal cutoffs of ADC= 0.68 × 10-3 (mm2/s) and D =0.74.×10-3 (mm2/s).Discussion and Conclusion
For the NPC patients who experienced LRF, ADC, and D histograms tend to show sharper peaks compared to patients who experienced favorable response, indicating varying tumor cellularity between the groups. The change in K value indicates subtle difference in tissue microstructure in NPC patients with and without LRF. Kaplan-Meier analysis demonstrated that the pretreatment ADC and D of the primary tumor were significant apriori predictors of LRF in NPC patients. After appropriate validation in a larger NPC population, these findings may be useful for adaptive radiotherapy.Acknowledgements
This work was supported by the MSKCC internal IMRAS grant and in part through the NIH/NCI Cancer Center Support Grant: P30 CA008748.References
1. Kamran SC, Riaz N, Lee N. Nasopharyngeal carcinoma. Surg Oncol Clin N Am. 2015;24(3):547-561.
2. Tan TH, Soon YY, Cheo T, et al. Induction chemotherapy for locally advanced nasopharyngeal carcinoma treated with concurrent chemoradiation: A systematic review and meta-analysis. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2018;129(1):10-17.
3. Ai QY, King AD, Law BK, et al. Diffusion-weighted imaging of nasopharyngeal carcinoma to predict distant metastases. Eur Arch Otorhinolaryngol. 2017;274(2):1045-1051.
4. Le Bihan D. Molecular diffusion, tissue microdynamics and microstructure. NMR in biomedicine. 1995;8(7-8):375-386.
5.Law BK, King AD, Bhatia KS, et al. Diffusion-Weighted Imaging of Nasopharyngeal Carcinoma: Can Pretreatment DWI Predict Local Failure Based on Long-Term Outcome? AJNR American journal of neuroradiology. 2016;37(9):1706-1712.
6. Jansen JF, Stambuk HE, Koutcher JA, Shukla-Dave A. Non-gaussian analysis of diffusion-weighted MR imaging in head and neck squamous cell carcinoma: A feasibility study. AJNR American journal of neuroradiology. 2010;31(4):741-748.
7. Le Bihan D, Breton E, Lallemand D, Grenier P, Cabanis E, Laval-Jeantet M. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology. 1986;161(2):401-407.
8. Lu Y, Jansen JF, Mazaheri Y, Stambuk HE, Koutcher JA, Shukla-Dave A. Extension of the intravoxel incoherent motion model to non-gaussian diffusion in head and neck cancer. Journal of magnetic resonance imaging : JMRI. 2012;36(5):1088-1096.
9.Jensen JH, Helpern JA. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR in biomedicine. 2010;23(7):698-710.
10. Paudyal R, Oh JH, Riaz N, et al. Intravoxel incoherent motion diffusion-weighted MRI during chemoradiation therapy to characterize and monitor treatment response in human papillomavirus head and neck squamous cell carcinoma. Journal of magnetic resonance imaging : JMRI. 2017;45(4):1013-1023.
11. ImageJ [computer program]. Bethesda, Maryland, USA: U. S. National Institutes of Health; 1997-2016.
12. R: A Language and Environment for Statistical Computing [computer program]. Vienna, Austria: R Foundation for Statistical Computing: URL http://www.R-project.org.; 2013.
Figures