3442
Inter- and intraobserver reproducibility of two different delineation of intravoxel incoherent motion in differentiating benign and malignant thyroid nodule1MR Department, Beijing Shijitan Hospital of Capital Medical University, Beijing, China, 2Philips Healthcare, Hong Kong, China, 3Beijing Friendship Hospital, Capital Medical University, Beijing, China
Synopsis
To compare the reproducibility and diagnostic performance of IVIM parameters derived from 3D whole-lesion (W-L ROI) and single-section (S-S ROI) delineation respectively . Forty-three patients with 46 pathologically confirmed thyroid nodules were involved. Reduced FOV DWI with 2D RF was employed to decrease the distortion. The ICC values of all IVIM parameters were higher with W-L ROI delineation than with S-S ROI delineation. The 95% limits of agreement (Bland-Altman plots) determined by W-L ROI revealed smaller absolute intra- and interobserver variability and the AUC of W-L ROI delineation was higher than S-S ROI according to ROC analysis.
Introduction
Some studies have demonstrated the potential of ADC to distinguish benign from malignant thyroid nodules, but the results are inconsistent, and some recent meta-analyses have shown that the diagnostic threshold results have considerable variability (0.36–2.56 × 10-3 mm2/s). The most likely cause of these phenomena were substantial variance in quantitative data, which might have been influenced by different b-values used, the heterogeneity in pathological characteristics, and the subjectivity of region of interest (ROI) delineation1. During the acquisition of quantitative data, the ROI size and positioning have considerable influences. For the whole-lesion (W-L) ROI method, freehand ROIs are drawn along the border of the tumour in consecutive slices to cover the entire tumour area. For the single-section (S-S) ROI method, a single freehand ROI is drawn on a single slice containing the largest available tumour area or multi-slices containing a solid area.
To the best of our knowledge, no published studies have compared the reproducibility of these two delineation methods in thyroid nodules. This study aimed to compare the reproducibility of intravoxel incoherent motion (IVIM) parameters (D, f and D*) derived from a W-L ROI and an S-S ROI and the diagnostic performance to distinguish malignant from benign thyroid nodules.
Methods
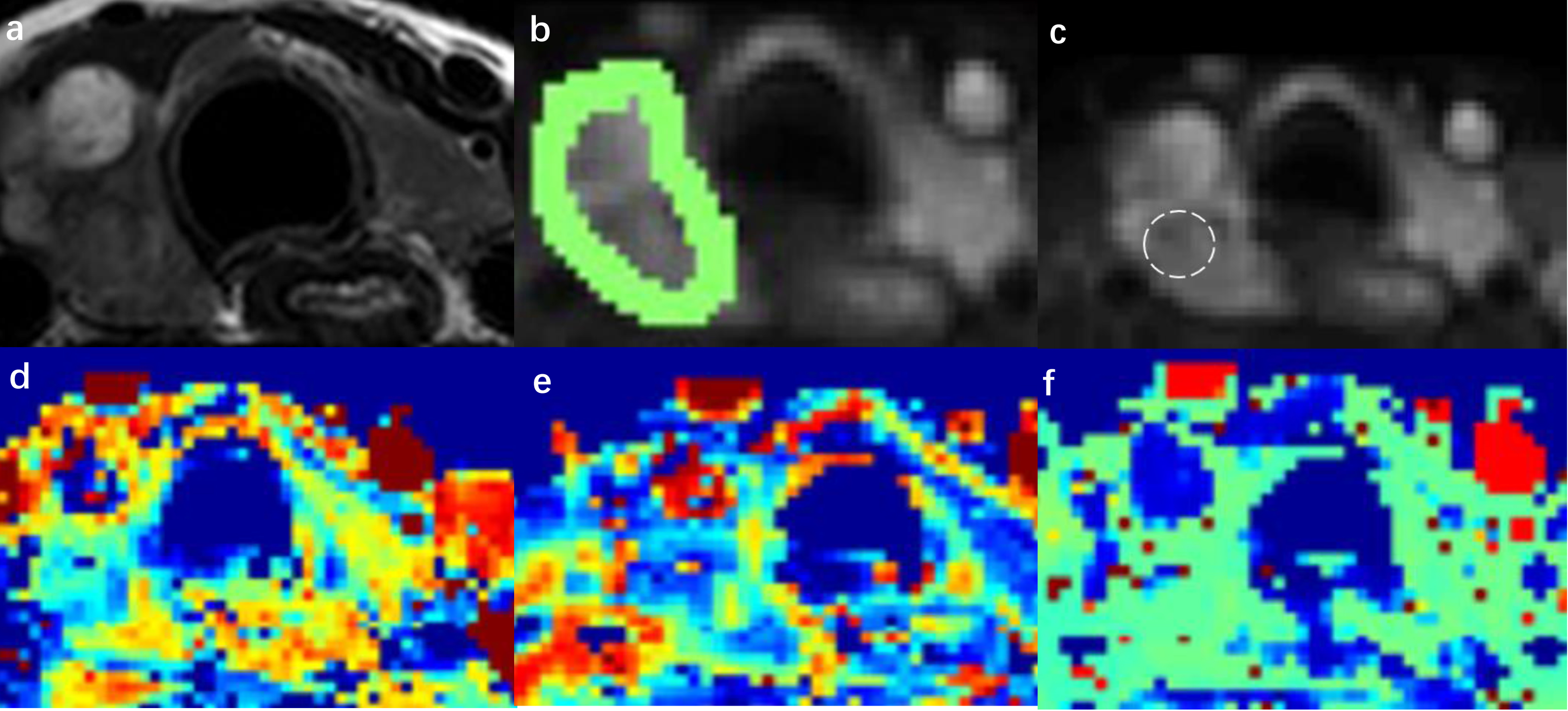
Forty-three patients (6 men, 37 women; mean age, 42 ± 11 years; age range, 18-68 years) with 46 pathologically confirmed thyroid nodules were involved . All patients underwent preoperative examinations (Philips 3.0T Ingenia, Philips Medical System, The Netherlands) with conventional imaging and reduced FOV DWI sequences using an 8-channel carotid coil. A reduced FOV DWI examination using 2D RF pulse for shorter echo train length to decrease the distortion was scanned with following parameters: TE/TR 69/1400ms; FOV 160x47mm; acquisition matrix 108x30; 10 slices with the thickness of 5mm and 1mm gap; NSA 4. Eight b-values (0, 20, 50, 100, 200, 400, 600, 990) were used. The non-linear fitting of the bi-exponential model was performed on Matlab. 3D W-L ROI was manually drawn on multiple slices to cover the whole nodule and S-S ROI was drawn as large as possible within the most solid tumour part (in the b = 0 s/mm2) in two independent tumour-containing slices. Two observers who were blinded to the clinical and histopathological data measured IVIM parameters values using W-L ROI and S-S ROI delineation respectively (Figure1), and repeated measurements were performed at an interval of four weeks by one radiologist. Intraclass correlation coefficients (ICC) and Bland-Altman plots were used to evaluate the intra- and interobserver variability. The mean values of all parameters in the malignant group and the benign group were compared by independent samples t-tests. Receiver operating characteristic (ROC) curves were generated to evaluate the diagnostic performance of these parameters. All statistical analyses were performed using MedCalc Online, version 16.2 (Medcalc Software, Mariakerke, Belgium) and SPSS (18.0 for Windows, SPSS, Chicago, IL). A P value < 0.05 indicated a statistically significant difference.Results
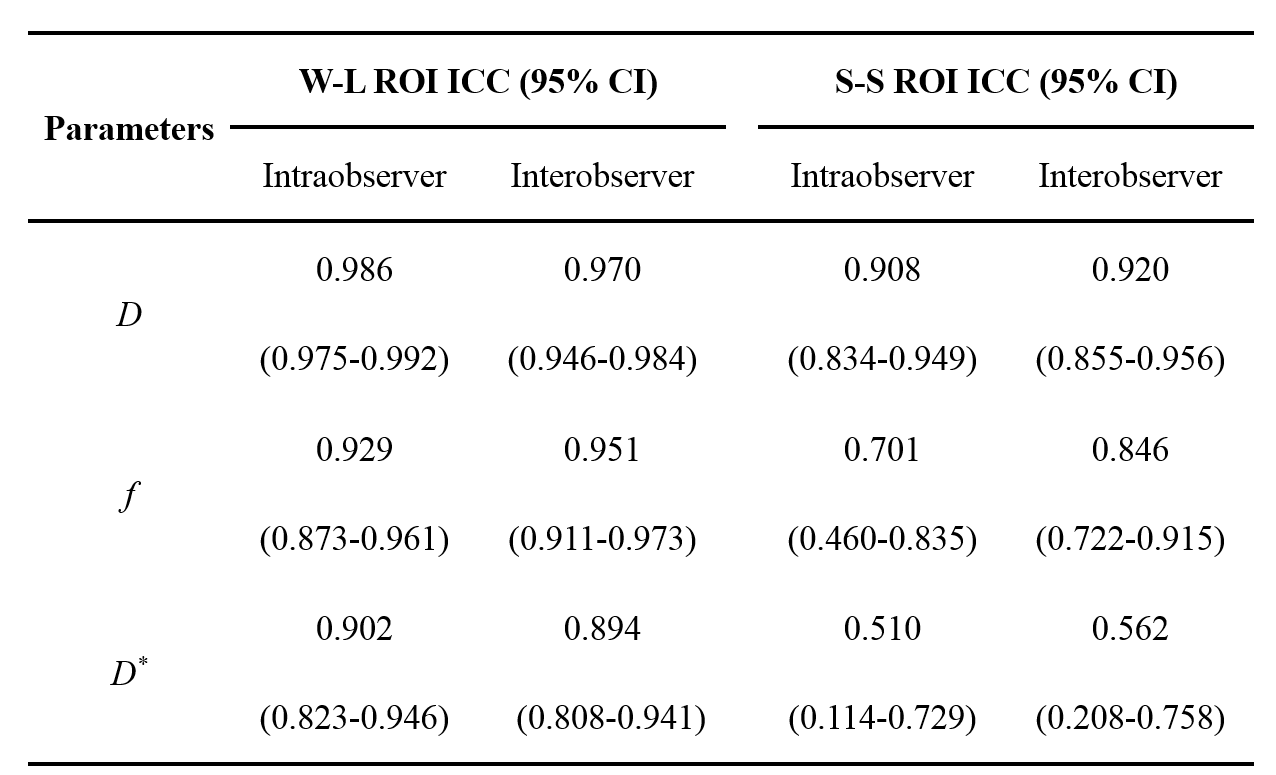
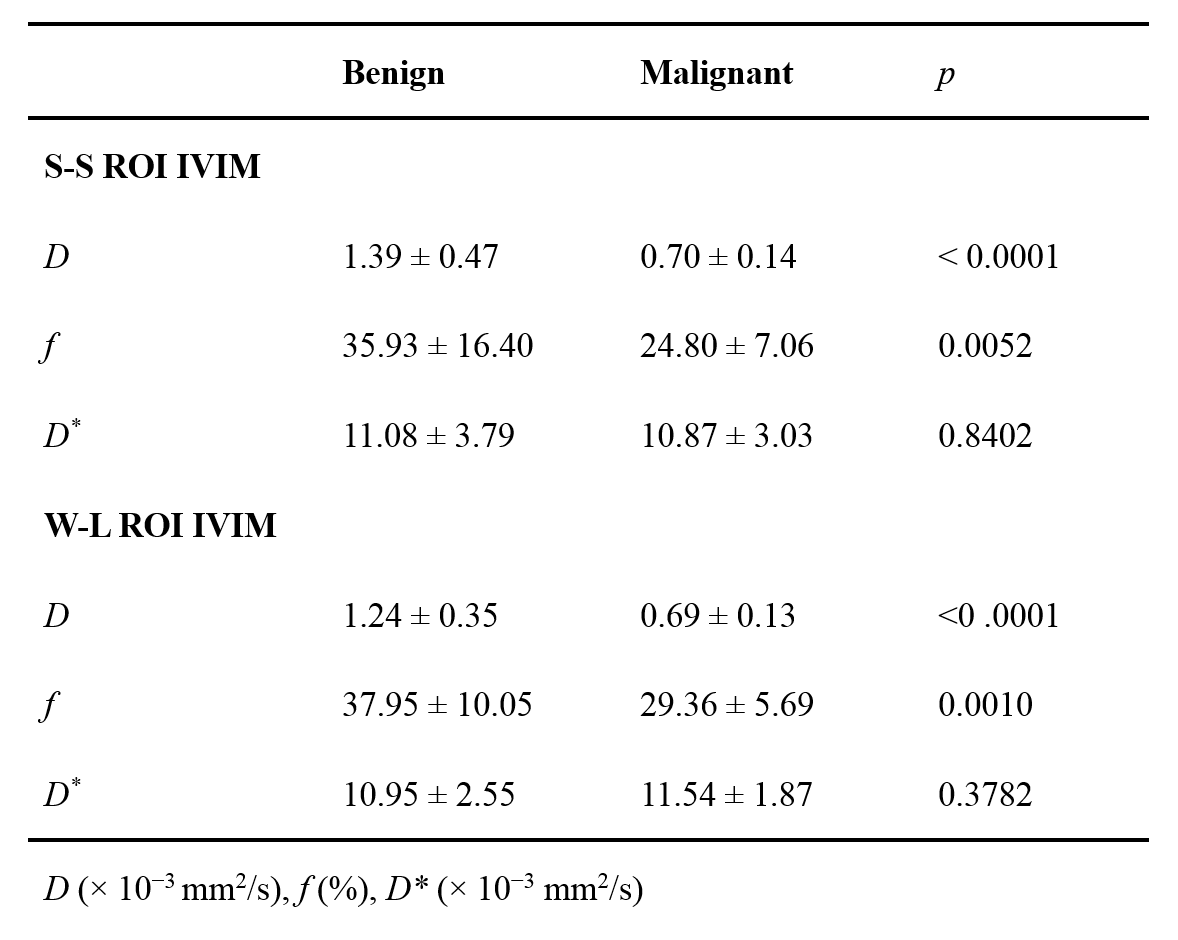
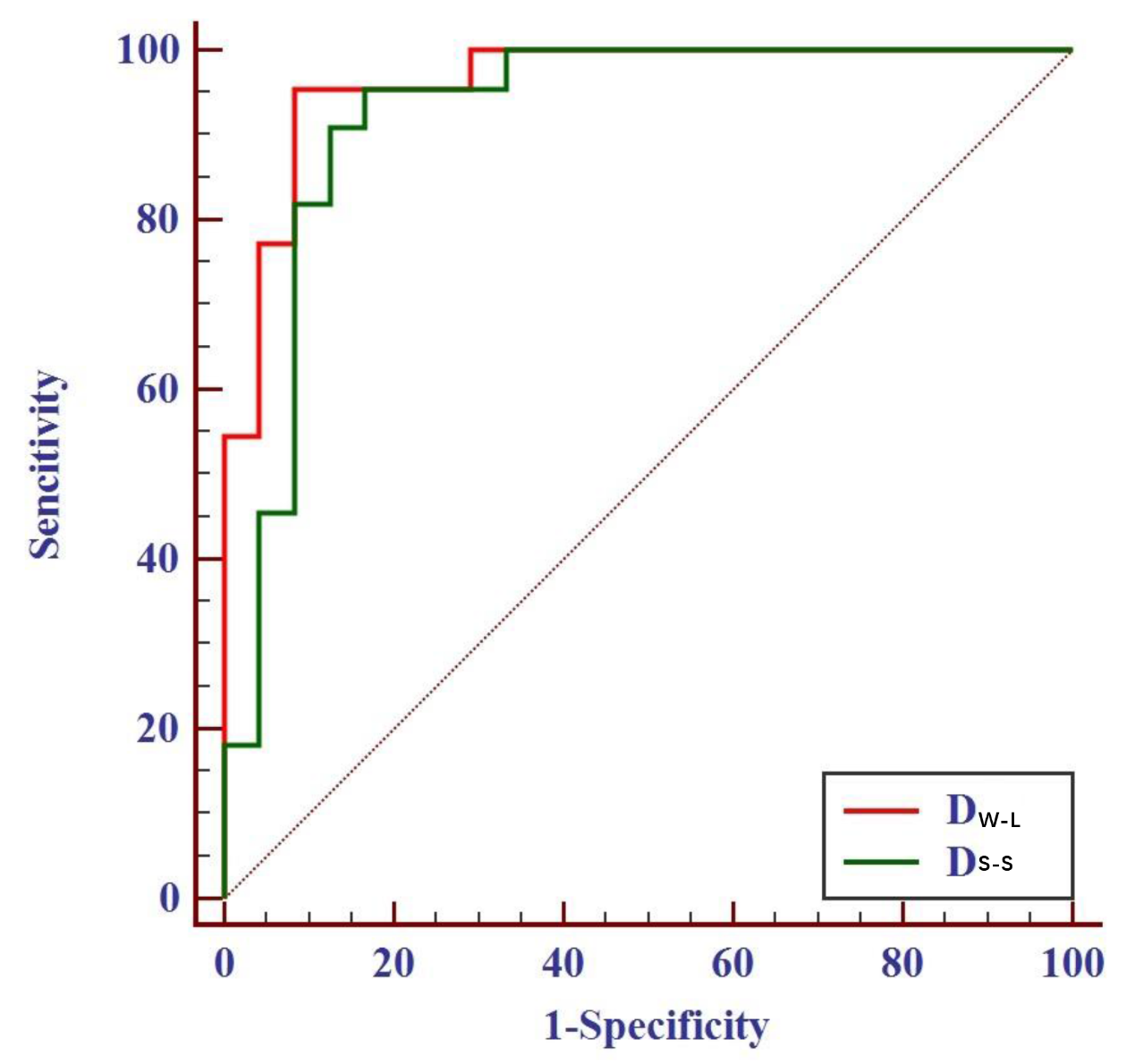
The pathological findings confirmed 24 benign nodules and 22 malignant nodules. The ICC values of all IVIM parameters were higher with W-L ROI delineation than with S-S ROI delineation, and excellent intra- and interobserver reproducibility were obtained (Table1). With Bland-Altman plots, the 95% limits of agreement of the IVIM parameters determined by W-L ROI revealed smaller absolute intra- and interobserver variability than those determined by S-S ROI. The results of independent samples t-tests for benign and malignant nodules are summarized in Table 2. Among three IVIM parameters derived from two ROI methods, D and f values were significantly lower in the malignant nodules than in the benign nodules. D value obtained from W-L ROI was the most powerful parameters for differentiating benign and malignant nodules [area under the ROC curve= 0.962] (Figure2).Discussion
This finding suggested that W-L ROI analysis might improve the assessment of tumours by capturing inherent intratumoural heterogeneity better. The results showed that all IVIM parameters derived from W-L ROI delineation were more reproducible than those derived from S-S ROI delineation, which was consistent with the findings of previous studies of other organs2,3. It is worth mentioning that especially D* and f values derived from W-L ROI showed excellent intra-and interobserver agreement when compared with S-S ROI analysis. The W-L ROI analysis was adopted in the present study for minimizing observer bias and obtaining more reliable results. Using W-L ROI delineation could reduce artificial influences thus providing a strong basic work for future multi-centre large sample and stratification research.Conclusion
IVIM measurements derived from W-L ROI delineation in thyroid nodules was a robust method with excellent reproducibility for differentiating benign from malignant nodules.Acknowledgements
No acknowledgement found.References
- Lambregts DM, Beets GL, Maas M, et al. Tumour ADC measurements in rectal cancer: effect of ROI methods on ADC values and interobserver variability. Eur Radiol 2011; 21:2567-2574.
- Nougaret S, Vargas HA, Lakhman Y, et al. Intravoxel Incoherent Motion-derived histogram metrics for assessment of response after combined chemotherapy and radition therapy in rectal cancer: initial experience and comparison between single-section and volumetric analyses. Radiology 2016; 280:446-454.
- Lee Y, Lee SS, Kim N, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of the liver: effect of triggering methods on regional variability and measurement repeatability of quantitative parameters. Radiology 2015; 274:405-415.
Figures