3441
Assessment of Traumatic Peripheral Nerve Injury and Carpal Tunnel Syndrome with Diffusion Tensor Imaging1Institute of Imaging Science, Vanderbilt University, Nashville, TN, United States, 2Plastic Surgery, Vanderbilt University Medical Center, Nashville, TN, United States, 3Biomedical Engineering, Vanderbilt University, Nashville, TN, United States, 4Radiology and Radiological Sciences, Vanderbilt University Medical Center, Nashville, TN, United States
Synopsis
Clinical management following traumatic peripheral nerve injury and carpal tunnel release surgeries requires physicians to rely on qualitative measures from patient history and physical exams. The resulting delays in clinical decision-making can lead to a negative impact on patient outcomes because the regeneration of nerves must occur in a timely fashion to avoid permanent muscle atrophy and loss of sensorimotor function. The current study aims to test the feasibility of performing diffusion tensor imaging in the nerves of the wrist to provide a noninvasive and reliable tool that can monitor patient outcomes and improve clinical decision-making after surgical interventions.
Introduction
Traumatic peripheral nerve injury (TPNI) occurs in 5% of level 1 trauma cases and results in approximately 100,000 surgeries per year [1]. TPNI has also become prevalent in recent military missions, as advancements in safety equipment focus on preventing lethal attacks rather than non-lethal, peripheral injuries. Presently, clinical management following TPNI requires physicians to “wait and watch” for weeks to months and rely on qualitative measures from patient history/physical exam. These delays may have a negative impact on outcomes because re-innervation must occur in a timely fashion to prevent permanent loss of sensorimotor function. Diffusion tensor imaging (DTI) provides a noninvasive approach to probe tissue microstructure throughout the recovery process by measuring the effect of tissue barriers on the apparent diffusion of water molecules [2]. Previous work has shown that DTI of the distal nerves of the wrist is feasible and reports on myelin and axon pathologies [3-4]. The long-term aim of this project is to employ DTI in the wrist nerves of TPNI as a quantitative, early measure of surgical success, as almost 40% of surgical repairs fail following TPNI [5]. The current study aims to test the sensitivity of performing DTI in a cross-section of TPNI and acquire preliminary longitudinal data. Additional patients with milder carpal tunnel syndrome (CTS) and release surgeries were also evaluated for comparison.Methods
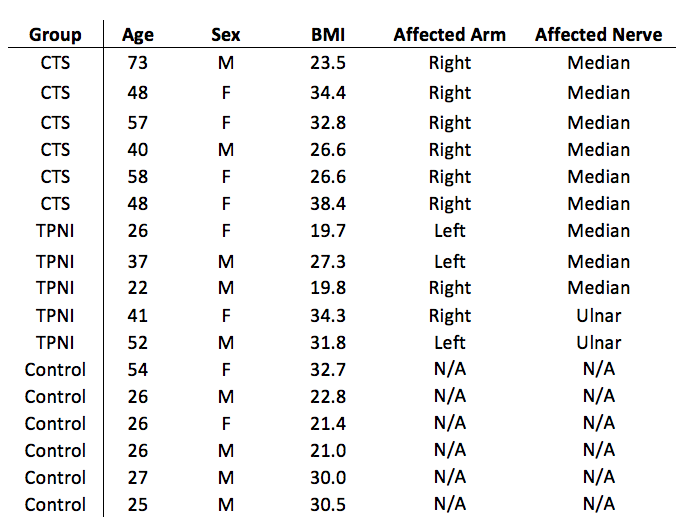
Subjects: Six patients with TPNI and five patients with CTS were included in this study. All TPNI patients underwent surgical repairs of the fully lacerated median or ulnar nerves, while CTS patients underwent carpal tunnel release surgery to relieve nerve compression. All patients underwent MRI one to three months after surgical repair. Longitudinal data were collected in three-month intervals after baseline scanning in three patients with TNPI. Six age-, sex-, and BMI-matched controls were scanned for comparisons. Descriptive statistics for all subjects can be found on Figure 1. Data acquisition: Subjects were imaged in the prone position with one arm extended above the head (i.e., “superman” position) with a 3.0-T Philips Achieva MR scanner. An 8-channel wrist coil was used for RF reception in all subjects expect one, where a larger 16-channel knee coil was used due to a cast covering the arm. High-resolution, single-shot DTI scan was performed at a slice thicknesses of 4-mm with 10-16 slices in each subject. Additional parameters included: resolution = 0.75x0.75x4 mm3 (wrist coil) or 1.25x1.25x8 mm3 (knee coil), TR/TE = 3000/53 ms, averages = 12, 16 directions, max b-factor of 800 s/mm2, and scan time ≈ 11 minutes. Data analysis: Image registration/tensor estimation was performed in MATLAB. Regions of interest (ROIs) were manually selected on all slices for the median/ulnar nerves, and mean slice-wise diffusion values were estimated. Finally, fibertracking was accomplished using seed-points in the proximal and distal slice, way-points halfway between seed-points, and a curve/FA threshold of 30˚/0.3.Results
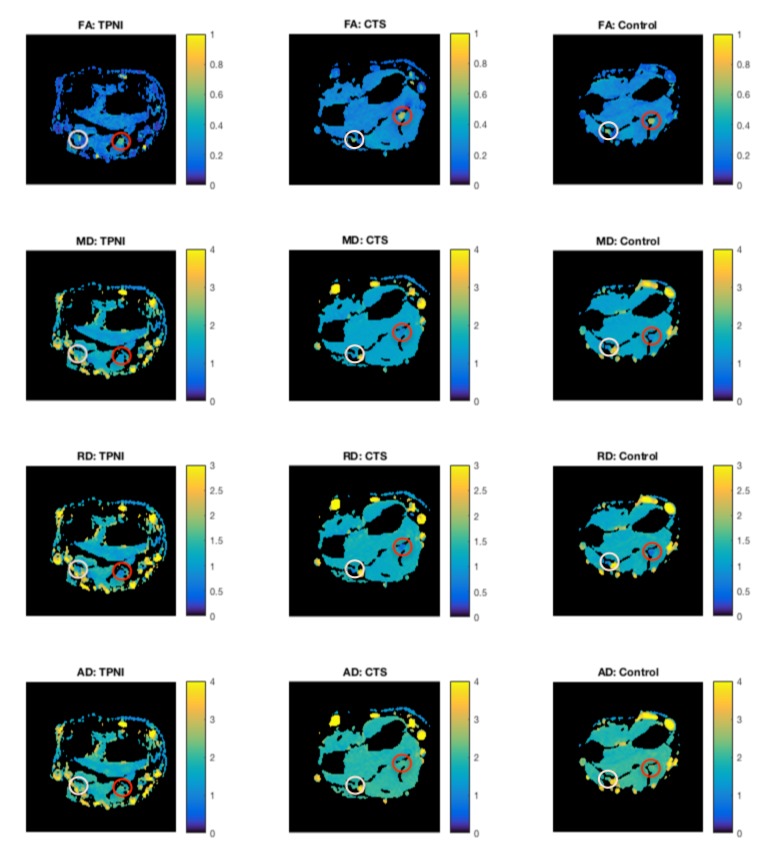
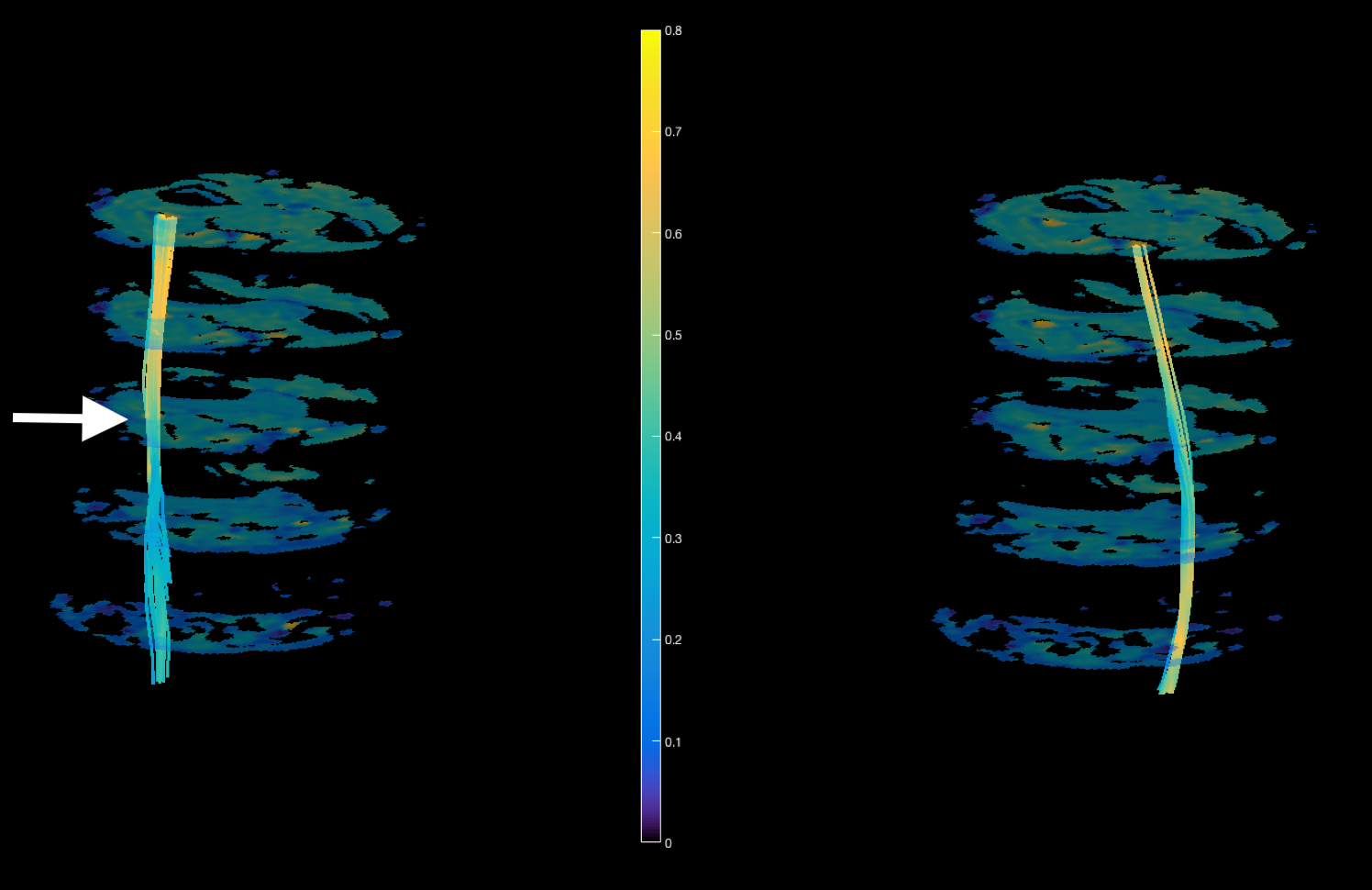
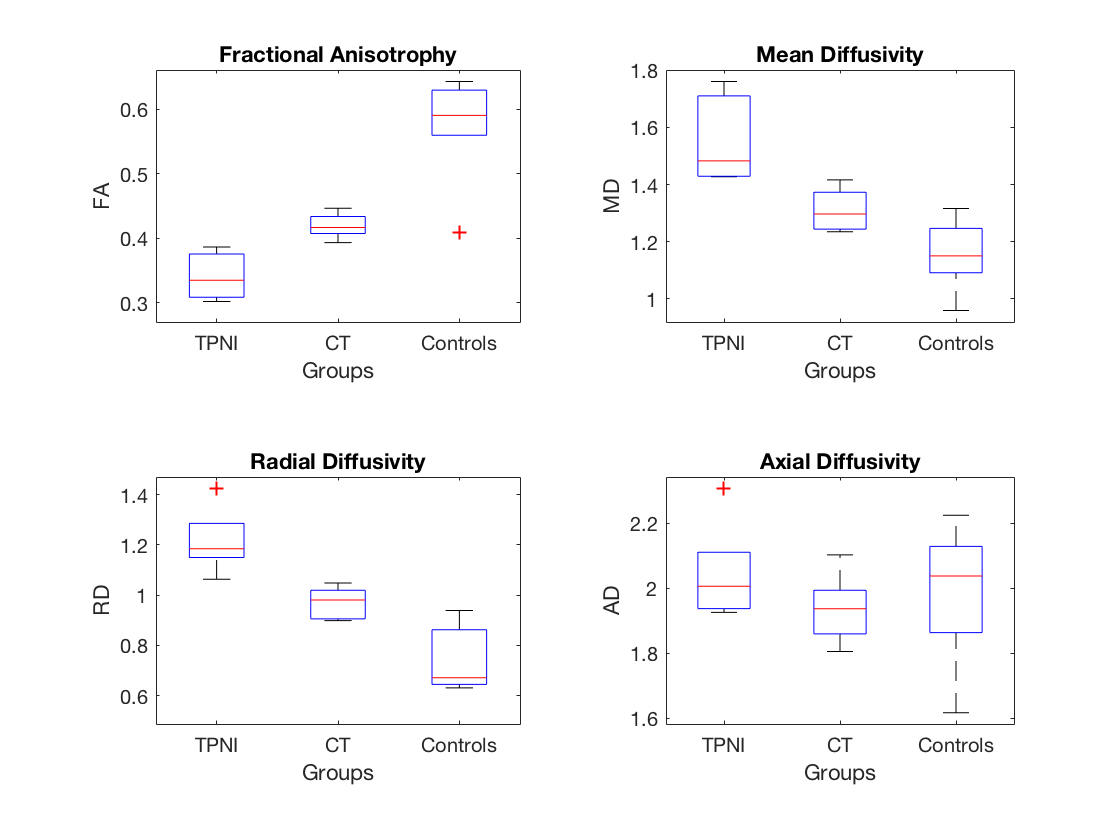
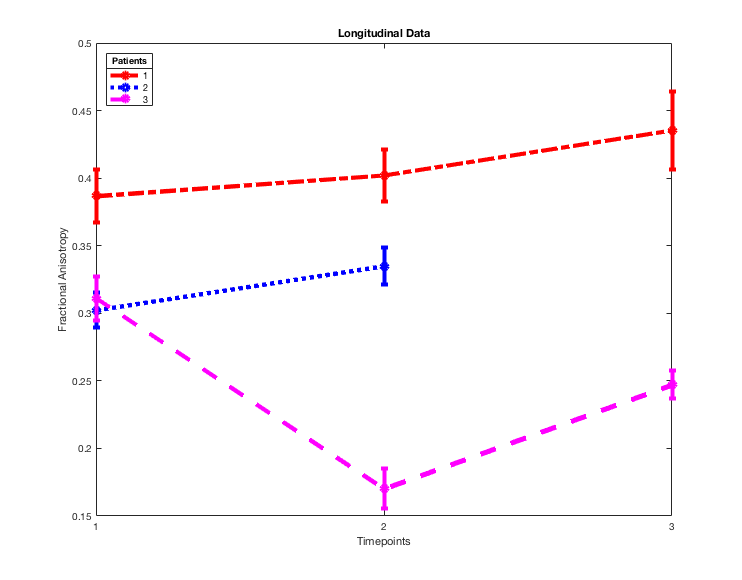
Figure 2 shows representative FA maps from each cohort, while Figure 3 shows representative fibertracking results, which revealed a drop in FA for the injured median nerve distal to the injury site that was not observed in the uninjured ulnar nerve in the same arm. Group comparisons were conducted via nonparametric Mann-Whitney U-tests for each analysis. Analysis of TPNI and control subjects found significant differences for FA (p = 0.008), MD (p = 0.008), and RD (p = 0.008). Analysis of CTS and control subjects also found significant differences for FA (p = 0.026), MD (p = 0.041), and RD (p = 0.008). The differences here for FA/MD/RD between the TPNI and CTS groups likely reflects the milder injury occurring in CTS. A boxplot of all groups and diffusion measures can be seen on Figure 4, which suggests our findings for FA in TPNI and CTS are driven by radial diffusivity. Case-based analyses were done for longitudinal TPNI patients (Figure 5). Patients 1 and 2 showed an increase in FA over time, while Patient 3 had a decrease from timepoint 1 to timepoint 2, and an increase from timepoints 2 to 3, indicating the inhomogeneity of injury severity and/or recovery.Discussion & Conclusion
DTI of the wrist is feasible and sensitive to TPNI and CT in the peripheral nerves. Additionally, we were able to differentiate between controls, CT, and TPNI groups based on our diffusion metrics. Further work will focus on i) obtaining data in a larger cohort of patients and matched controls; ii) refining the scan protocol, specifically with coil selection and subject position on the table; iii) modeling edema; and iv) tracking patients over time to determine the ability of DTI to track change.Acknowledgements
R01 NS097821, MR 150075, W81-XWH-15-JPC-8/CDRMP-NMSIRA, and T32 EB014841-05 for funding.References
1. Chhabra A, Ahlawat S, Belzberg A, Andreseik G. Peripheral nerve injury grading simplified on MR neurography: As referenced to Seddon and Sunderland classifications. Indian Journal of Radiology & Imaging. 2014;24(3):217-24.
2. Naraghi A, Awdeh H, Wadhwa V, Andreisek G, Chhabra A. Diffusion tensor imaging of peripheral nerves. Seminars in Musculoskeletal Radiology. 2015;19(02):191-200.
3. Heckel A, Weiler M, Xia A, Ruetters M, Pham M, et al. Peripheral nerve diffusion tensor imaging: Assessment of axon and myelin sheath integrity. PLOS ONE. 2015;10(6):e0130833.
4. Jeon T, Fung MM, Koch KM, Tan ET, Sneag DB. Peripheral nerve diffusion tensor imaging: Overview, pitfalls, and future directions. Journal of Magnetic Resonance Imaging. 2018;47:1171-1189.
5. Ruijs AC, Jaquet JB, Kalmijn S, Giele H, Hovius SE. Median and ulnar nerve injuries: A meta-analysis of predictors of motor and sensory recovery after modern microsurgical nerve repair. Plastic and Reconstructive Surgery. 2005;116:484-494.
Figures