3438
Comparison of IVIM Model, Kurtosis Model and IVIM-Kurtosis Model for the Grading of Hepatocellular Carcinoma1Beijing Hospital, Beijing, China
Synopsis
IVIM model and DKI model cover different aspects of diffusion, thus a combined IVIM-DKI model might describe diffusion in perfused biological tissues more accurately. The aim of the study was to quantitatively compare the potential of various parameters obtained from IVIM model, Kurtosis model and IVIM-Kurtosis model in the grading of hepatocellular carcinoma (HCC). We enrolled 24 HCC patients who underwent multiple b values Diffusion-Weighted Imaging (DWI) with subsequent pathological confirmation. Our results showed that all three models could differentiate high-grade HCC from low-grade HCC and IVIM-Kurtosis model may be superior to IVIM model.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignant tumor of the liver. The histological grade of HCC is heavily associated with the prognosis, and it is one of the independent predictive factors for recurrence and long-term survival after hepatic curative resection in patients with HCC.1,2 Some studies showed,3,4 IVIM model and Kurtosis model could predict histological grade of HCC. However, no studies have been reported that were designed to evaluate the diagnostic performance of IVIM-Kurtosis model in the predicting histological grade of HCC, compared with IVIM model and Kurtosis model.Methods
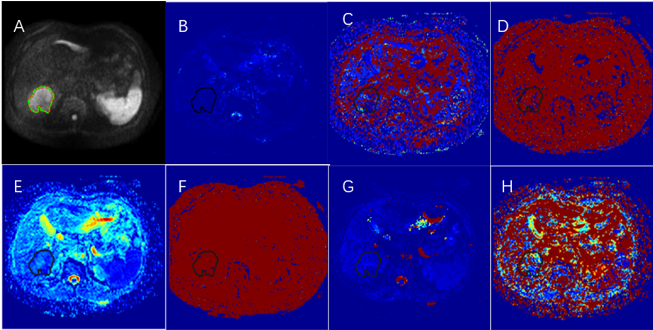
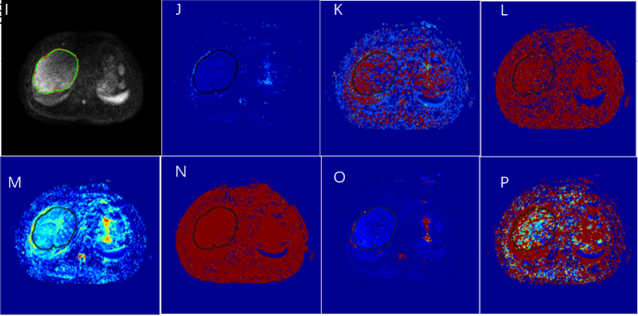
Between May 2017 and April 2018, 24 consecutive patients with pathologically confirmed HCC were enrolled, who underwent DWI with 9 values (0,20,50,100,200,500,1000,1500,2000 s/mm2) on a 3.0-T MRI scanner. DWI were analyzed by three model, including IVIM model (diffusion coefficient(DIVIM), pseudo diffusion coefficient (D*IVIM), perfusion fraction (fIVIM)), Kurtosis model (diffusion coefficient (DKurtosis), kurtosis(KKurtosis) and IVIM-Kurtosis model(diffusion coefficient(DIVIM-Kurtosis), pseudo diffusion coefficient (D*IVIM-Kurtosis), perfusion fraction(fIVIM-Kurtosis), kurtosis (KIVIM-Kurtosis)). All values were compared between high-grade and low-grade HCC by using a Student t test. Receiver operating characteristic analysis was used for statistical evaluations.Results
DIVIM, DIVIM-Kurtosis, D*IVIM-Kurtosis values were significantly lower in high-grade HCC than in low-grade HCC (P=.016, P=.021, and P=.009, respectively). KKurtosis and KIVIM-Kurtosis values were significantly higher in high-grade HCC than in low-grade HCC (P=.026, and P <.001, respectively). The area under the curve (AUC) of DIVIM, KKurtosis, DIVIM-Kurtosis, D*IVIM-Kurtosis and KIVIM-Kurtosis was 0.719, 0.828, 0.992,0.820 and 0.945, respectively. Both DIVIM-Kurtosis (AUC=0.992) and KIVIM-Kurtosis (AUC =0.945) had significantly greater AUC values than DIVIM (AUC = 0.719) in the differentiation of low-grade and high-grade HCC (P <.05). The area under the curve (AUC) of IVIM-Kurtosis model, IVIM model and Kurtosis model was 1.000,0.805 and 0.883, respectively. IVIM-Kurtosis model was superior to IVIM model in the discrimination of low-grade and high-grade HCC (P <.05).Discussion
In this study, we performed comparisons on the diagnostic accuracy on HCC using IVIM model, Kurtosis model and IVIM-Kurtosis model, which may help to reveal the clinical applicability of these models. The IVIM model is able to separate the molecular perfusion component from diffusion and offers both pure molecular diffusion parameters (DIVIM) as well as perfusion-related diffusion parameters (D*IVIM and fIVIM).5 The DKI model is able to detect the information related to the microstructural tissue heterogeneity.6 In our study, DIVIM from IVIM model and KKurtosis from Kurtosis model values could be used to discriminate between high and low-grade HCC: DIVIM values were significantly lower in high-grade HCC than in low-grade HCC (P=.016), KKurtosis values were significantly higher in high-grade HCC than in low-grade HCC (P=.026). The results were consistent with others.3,4 As HCC becomes more poorly differentiated during hepatocarcinogenesis, cellular density and nuclear-to-cytoplasmic ratios increase, while the architecture becomes more complicated. Therefore, the increased cellular density in high-grade HCC should result in a decrease in DIVIM values and the architecture becomes more complicated should result in an increase in KKurtosis values.
As compared to IVIM model and Kurtosis model, the IVIM-Kurtosis model might combine the two features of IVIM model and Kurtosis model, not only reflected the tissue diffusion but also heterogeneity. In the IVIM-Kurtosis model, all parameters except the f value were significantly different between high and low-grade HCC. When looking at the receiver operating characteristic curves in discriminating high-grade HCC from low-grade HCC, the AUC values for both DIVIM-Kurtosis and KIVIM-Kurtosis were significantly greater than DIVIM (P <.05). Besides the comparisons of individual parameters, the utility of the three models in HCC diagnosis was also compared to find out which model may provide the most accurate information. We made these comparisons to find out whether IVIM-Kurtosis model would have better diagnostic accuracy than IVIM model and Kurtosis model, and which model showed the best diagnostic accuracy. IVIM-Kurtosis model showed higher AUCs than IVIM model and Kurtosis model, but significant difference was only observed between IVIM-Kurtosis and IVIM. Thus, it may be beneficial to use IVIM-Kurtosis model in the diagnosis of HCC for the better diagnostic accuracy compared to IVIM model. Some study showed,7 that the inclusion of kurtosis in the well-established IVIM model of diffusion has several effects: First, curve fitting to the signal decay is improved, thereby potentially improving the informative value of the calculated parameters. Second, the true diffusion coefficient D as well as the pseudo-diffusion coefficient D* increase accompanied by a decrease in the perfusion fraction f. In the present study, IVIM-Kurtosis model seemed to have some advantages over the two separate models.
Conclusion
IVIM model, Kurtosis model and IVIM-Kurtosis model could discriminate between high and low-grade HCC. IVIM-Kurtosis model may be superior IVIM model in the differentiation of low-grade and high-grade HCC.Acknowledgements
No acknowledgement found.References
1.Clark T, Maximin S, Meier J, et al. Hepatocellular Carcinoma: Review of Epidemiology, Screening, Imaging Diagnosis, Response Assessment, and Treatment. Curr Probl Diagn Radiol.2015;44(6):479-486.
2.Parkin DM. Global cancer statistics in the year 2000. LANCET ONCOL. 2001;2(9):533-543.
3. Zhu S, Liu Y, Wei Y, et al. Intravoxel incoherent motion diffusion-weighted magnetic resonance imaging for predicting histological grade of hepatocellular carcinoma: Comparison with conventional diffusion-weighted imaging. WORLD J GASTROENTERO .2018;24(8):929-940.
4. Wang WT, Yang L, Yang ZX, et al. Assessment of Microvascular Invasion of Hepatocellular Carcinoma with Diffusion Kurtosis Imaging. RADIOLOGY. 2018;286(2):571-580.
5. Le Bihan D. Intravoxel incoherent motion perfusion MR imaging: a wake-up call. RADIOLOGY. 2008;249(3):748-752.
6. Jensen JH, Helpern JA, Ramani A, et al. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. MAGN RESON MED. 2005;53(6):1432-1440.
7. Wurnig MC, Kenkel D, Filli L, et al. A Standardized Parameter-Free Algorithm for Combined Intravoxel Incoherent Motion and Diffusion Kurtosis Analysis of Diffusion Imaging Data. INVEST RADIOL .2016;51(3):203-210.
Figures