3424
White Matter Microstructural Alternations in Neuropsychiatric Systemic Lupus Erythematosus With Normal Appearing Brain Using Diffusion Tensor Imaging1Department of Radiology, Taichung Veterans General Hospital, Taichung, Taiwan, 2College of Medicine, China Medical University, Taichung, Taiwan, 3Department of Medical Imaging and Radiological Sciences, Central Taiwan University of Sciences and Technology, Taichung City, Taiwan, 4College of Human Development and Health, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan, 5Department of Thanatology and Health Counseling, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan, 6Department of Biomedical Engineering, Hung Kuang University, Taichung City, Taiwan
Synopsis
Systemic lupus erythematosus (SLE) patient has neuropsychiatric signs and symptoms, called neuropsychiatric SLE (NPSLE), usually with increased mortality and morbidity rates. There was little known about pathogenic mechanisms leading to neuropsychiatric symptoms in SLE. The aims of this study attempt to investigate diffusion tensor imaging (DTI) in detection of white matter micro-structural alternations for NPSLE patients, who had normal appearing brain in conventional MRI. By using the TRACULA analysis, we found significant differences of mean diffusivity (MD) and fraction anisotropy (FA) in several important nerve tracts between NPSLE patients and normal subjects, which would be helpful in understanding the mechanisms of NPSLE.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease with multi-organ involvement. Once patient has neuropsychiatric signs and symptoms (eg. stroke, movement disorder and psychosis), called neuropsychiatric SLE (NPSLE), the mortality and morbidity rates would be significantly increased [1]. A variety of brain findings in NPSLE had been observed, ranging from normal to predominantly global atrophy and focal or multiple nonspecific white matter disease [2]. However, there was little known about pathogenic mechanisms leading to NP symptoms in SLE, whether it is caused by ischemia or auto-antibody mediated neuronal loss. The aims of this study attempt to investigate early microstructual alternations in NPSLE patients by using diffusion tensor imaging (DTI).Methods
In this study, 31 patients with NPSLE (M/F: 4/27; 39.93±10.77 y/o) were enrolled with criteria of no abnormal brain lesion in conventional MR imaging. Another 33 healthy controls with age- and sex-match (M/F: 4/29; 37.88±7.99 y/o) were also collected for comparison. A battery of standardized tests is used to measure different areas of cognition, such as attention, concentration, cognitive speed, executive function/abstract problem‐solving and motor function, which including: the Beck Depression Inventory (BDI), neuropsychiatric inventory (NPI) , Taiwan version of the Montreal Cognitive Assessment (T-MoCA), frontal assessment battery (FAB), and the Taiwan version of the Mini Mental State Examination (T-MMSE), as shown in Table1. DTI data were acquired on a 1.5T Siemens MR system with following parameters: TR/TE=10000/107ms, b-value=1000 s/mm2, 30 directions, NEX=3 and voxel size=2*2*2mm3. Whole brain tracts of the mean diffusivity (MD), fraction anisotropy (FA), axial diffusivity (AD) and radial diffusivity (RD) were carried out using FMRIB Software Library v5.0 (FSL) and TRActs Constrained by UnderLying Anatomy (TRACULA). The statistical analysis of the DTI indices of 68 ROIs were performed using a parametric permutation test and P<0.05 for significance. Subsequently, partial Pearson correlation analyses were performed to correlate the clinical evaluations with the regional DTI values within patient groups. TRACULA pipeline was followed to show 18 brain tracts differences of both FA and MD in these two groups and P<0.05 for significance.Results
Table 2 showed the detail areas with significantly different DTI indexes in two study groups. The results showed significantly lower FA in left corticospinal tract (L_CST) and right inferior longitudinal fasciculus (R_ILF) in NPSLE group than the normal subjects. MD in left anterior thalamic radiations (L_ATR), left cingulum (L_CCG), right corticospinal tract (R_CST), right superior longitudinal fasciculus (R_SLFP), right and left superior longitudinal fasciculus (R_ and L_SLFT) were significantly higher in NPSLE patients than the normal subjects. There were also significant differences of AD in R_SLFP and R_SLFT, and RD in bilateral ATR, L_CST and L_SLFP. Figure 1 (a) and (b) showed the areas with significantly different in FA and MD in TRACULA. Figure 1 (c) showed the integrity of 18 fibers in two groups. The results also revealed their associations with impairment of some specific motor and cognitive functions.Conclusions
In this experiment by TRACULA analysis, we could see the significant differences of white matter DTI indexes in bilateral cerebral hemispheres between NPSLE patients with normal appearing brain and normal subjects. Although the pathogenic process responsible for white matter alterations in NPSLE patients is still unknown, our preliminary results of altered mean FA, MD, AD and RD in the regional WM would indicate that there is micro-structural neuronal damage in NPSLE patients with no gross abnormality in the conventional brain MRI examinations, which were also in accordance with the previous studies [3,4,5]. In conclusion, our study revealed micro-structural alternations in grossly normal appearing brain of NPSLE patients. The finding would be much helpful for further investigation of the pathogenic mechanisms leading to NP symptoms in SLE.Acknowledgements
Nil.References
1. ACR AD HOC COMMITTEE ON NEUROPSYCHIATRIC LUPUS NOMENCLATURE. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. 1999;42:599–608 2. Kaichi Y, Kakeda J, Moriya J, Ohnari N, Saito K, Tanaka Y, et al. Brain MR Findings in Patients with Systemic Lupus Erythematosus with and without Antiphospholipid Antibody Syndrome. AJNR 2014;35:100-105. 3. Kozora E, Filley CM. Cognitive dysfunction and white matter abnormalities in systemic lupus erythematosus. J Int Neuropsychol Soc. 2011;17(3):385–92. 4. Shapira-Lichter I, Weinstein M, Lustgarten N, Ash E, Litinsky I, Aloush V, Anouk M, Caspi D, Hendler T, Paran D. Impaired diffusion tensor imaging findings in the corpus callosum and cingulum may underlie impaired learning and memory abilities in systemic lupus erythematosus. Lupus. 2016;25(11):1200–8. 5. Emmer BJ, Veer IM, Steup-Beekman GM, Huizinga TW, van der Grond J, van Buchem MA. Tract-based spatial statistics on diffusion tensor imaging in systemic lupus erythematosus reveals localized involvement of white matter tracts. Arthritis Rheum. 2010;62(12):3716–21
Figures

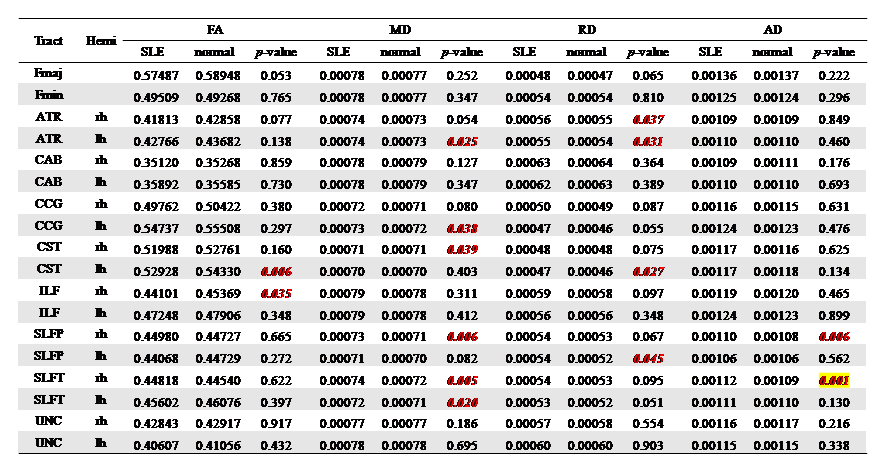
Table 2: Comparison of fractional anisotropy (FA), mean (MD), axial (AD), and radial (RD) diffusivity for the nerve tracts between NPSLE patients with normal appearing brain and normal subjects.
Note: Depicted are fractional anisotropy (FA), mean (MD), axial (AD), and radial (RD) diffusivity for each tractacross the scan interval. FMaj = Forceps Major, FMin = Forceps Minor, ATR = Anterior Thalamic Radiation, CAB = Cingulum Angular Bundle,CCG = Cingulum Cingular Bundle, CST = Corticospinal Tract, ILF = Inferior Longitudinal Fasciculus, SLFP = Superior Longitudinal Fasciculus Parietalpart, SLFT = Superior Longitudinal Fasciculus Temporal part, UNC = Uncinate Fasciculus. Bonferroni-corrected at factor of 18, p values are significantp = 0.003.
