3418
High-Resolution FLAIR DTI Tractography of the Fornix in Multiple Sclerosis1Biomedical Engineering, University of Alberta, Edmonton, AB, Canada
Synopsis
Diffusion tensor imaging (DTI) tractography of the human fornix is biased by partial volume effects from cerebrospinal fluid (CSF) due to its small bundle size and intra-ventricular location, even when using high spatial resolution. These errors in diffusion parameter estimation and tracking of the fornix will worsen with axonal loss in multiple sclerosis (MS). Here we demonstrate the superiority of FLAIR-DTI, even when compared to high-resolution 1.5 mm isotropic DTI, to mitigate CSF contamination of fornix tractography in MS and healthy volunteers. FLAIR-DTI yields more accurate diffusion metrics in both cohorts, and still shows abnormal fornix in MS.
Introduction
The limbic white matter (WM) tracts, particularly the fornix due to its role in memory1, have been the focus of diffusion tensor imaging (DTI) tractography studies in multiple sclerosis (MS)2,3. They have shown diffusion abnormalities (e.g. lower fractional anisotropy, FA; higher mean diffusivity, MD) which have been associated with impaired cognition in MS4. However, these tract diffusion metrics can be contaminated by partial volume effects5 from the adjacent isotropic and rapidly diffusing cerebrospinal fluid (CSF) due to the intraventricular location and small bundle thickness of the fornix. Thus, inaccurate results and premature streamline terminations can occur with atrophy of the fornix and the acquisition of typical low spatial resolution (e.g., 2 mm isotropic, 8 mm3 voxels). Inversion recovery FLAIR-DTI can suppress CSF and improve fornix tractography6, but it has not yet been used in MS. The purpose here was to evaluate the fornix in MS using two DTI protocols for tractography: (i) high-resolution 1.5 mm isotropic (3.4 mm3) voxels without FLAIR and (ii) FLAIR-DTI also with small 3.3 mm3 voxels at 3T.Methods
Four MS patients (33-61 years; 2 relapsing-remitting, RRMS; 2 secondary-progressive, SPMS, all female) and five healthy female controls (32-67 years) underwent FLAIR-DTI and high-resolution (1.5 mm isotropic) non-FLAIR DTI on a 3T Siemens Prisma with a 64-channel head coil (pre-scan normalize off). FLAIR-DTI was acquired with 35 2 mm axial slices centered over the fornix, 1.28x1.28 mm2 in-plane resolution zero-filled to 0.64×0.64 mm2, GRAPPA R=2, TR 8900 ms, TE 67 ms, TI 2300 ms, FOV 240 mm, b=1000 s/mm2, 20 directions, 5 b0, and scan time 4:11 min. High-resolution non-FLAIR DTI was acquired with 90 1.5 mm axial slices with whole brain coverage, multi-band acceleration 2, 1.5x1.5 mm2 in-plane resolution zero-filled to 0.75×0.75 mm2, GRAPPA R=2, TR 4700 ms, TE 64 ms, FOV 220 mm, 30 directions for b= 1000 and 2000 s/mm2 (only b=1000 s/mm2 used here), 6 b0, scan time 6 min. Pre-processing included eddy current and subject motion correction and RESTORE calculation of the diffusion tensor (ExploreDTI). Deterministic tractography was performed with an FA threshold of 0.15, turning angle of 35˚ and minimum fiber length of 10 mm. “SEED” and “AND” ROIs were placed in the columns, body, and crura of the fornix6 and “NOT” ROIs were placed as needed to remove spurious fibres. FA, MD, and volume were measured per fornix (left/right combined). These were compared between FLAIR and non-FLAIR protocols with a paired t-test for each group and between MS and controls with a 2-sample t-test for each protocol.Results
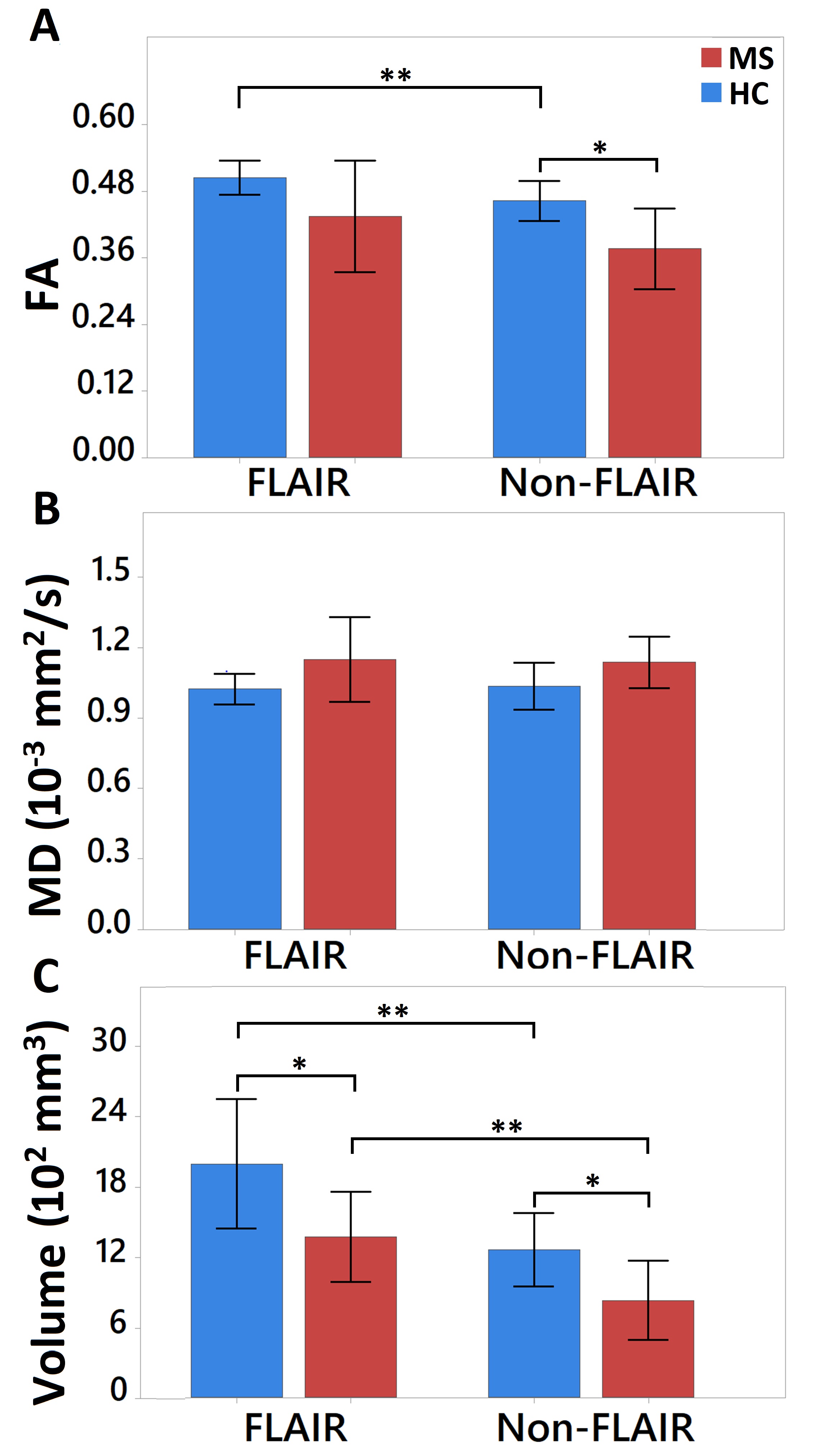
Even though both sequences had excellent in-plane resolution and fully depicted the fornix in all controls, the tractography was superior on FLAIR-DTI versus non-FLAIR DTI (Fig. 1). The healthy controls showed greater volumes and FA on FLAIR DTI than on the non-FLAIR DTI, but notably there were no significant MD differences (Fig. 2). One RRMS patient showed excellent fornix tracking in both protocols (Fig. 3A), while the other RRMS patient had a disrupted fornix on non-FLAIR DTI, which was alleviated on FLAIR DTI (Fig. 3B). Notably, the two SPMS patients had disrupted tractography on both DTI protocols, but the residual tracts were better identified on FLAIR DTI (Fig. 3C, D). These disruptions are caused by not reaching the tractography FA threshold due to either residual CSF or focal tract degradation. The FLAIR b0 showed extensive periventricular lesion areas in SPMS and seems to be related to the greater fornix disruptions although its anecdotal given the sample size (Fig. 3). As with controls, the MS patients had volumes that were systematically larger for the FLAIR-DTI than the non-FLAIR DTI even when the latter was acquired at 1.5 mm isotropic (Fig. 2). The percentage of tract volume reduction in MS to controls was similar for both protocols (FLAIR 31%, non-FLAIR 34%; Fig. 2C). The MS participants had significantly lower FA (19%) than the controls in non-FLAIR DTI, but it was not significant on FLAIR-DTI (Fig. 2A).Discussion and Conclusions
FLAIR-DTI yielded larger fornix reconstructions with tractography and more robust DTI parameters than non-FLAIR DTI, despite its 1.5 mm isotropic resolution. Even still, tract discontinuities of the fornix were present in 2/4 MS patients despite the use of small voxels and FLAIR. These partial volume effects and tractography failures will be worse for DTI resolutions typically acquired in MS (≥2 mm isotropic). High spatial resolution and CSF suppression can aid in ensuring that group differences or correlations with tractography-derived fornix parameters are not due to partial volume effects with CSF.Acknowledgements
This work was funded by the Canadian Institutes of Health Research (CIHR) while salary was provided by an endMS Studentship Award from the Multiple Sclerosis Society of CanadaReferences
1. Douet V, Chang L. Fornix as an imaging marker for episodic memory deficits in healthy aging and in various neurological disorders. Front Aging Neurosci. 2015; 7: 1–19.
2. Syc SB, Harrison DM, Saidha S, et al. Quantitative MRI Demonstrates Abnormality of the Fornix and Cingulum in Multiple Sclerosis. Mult Scler Int. 2013; 2013: 1–9.
3. Keser Z, Hasan KM, Mwangi B, et al. Limbic Pathway Correlates of Cognitive Impairment in Multiple Sclerosis. J Neuroimaging. 2017; 27: 37–42.
4. Kern KC, Gold SM, Lee B, et al. Thalamic–hippocampal–prefrontal disruption in relapsing–remitting multiple sclerosis. NeuroImage: Clinical. 2015; 8: 440–447.
5. Vos SB, Jones DK, Viergever MA, Leemans A. Partial volume effect as a hidden covariate in DTI analyses. NeuroImage. 2011; 55(4): 1566-1576.
6. Concha L, Gross DW, Beaulieu C. Diffusion Tensor Tractography of the Limbic System. AJNR Am J Neuroradiol. 2005; 26:2267–227.
Figures