3416
Difference in Tensor Metrics between the Survived and Infarcted Penumbra by Reperfusion in a Rat Model of Cerebral Ischemia1Neuroscience Research Center, Taipei Medical University, Taipei, Taiwan, 2Department of Radiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan, 3Translational Imaging Research Center, Taipei Medical University Hospital, Taipei, Taiwan, 4Department of Radiology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto, Japan, 5Department of Biomedical Imaging and Radiological Sciences, National Yang-Ming University, Taipei, Taiwan, 6Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung, Taiwan, 7Department of Medical Imaging, Taipei Medical University Hospital, Taipei, Taiwan
Synopsis
We demonstrated
Introduction
Intra-arterial (IA) mechanical thrombectomy (MT) has been proved showing beneficial on functional outcome and is announced as the new recommendation for the early management of acute ischemic stroke in 2018.1 It is acknowledged that by stringent selection of patients with much smaller initial infarct size and significant long-lasting penumbra, MT may show beneficial outcomes compared to intravenous administration of tPA along for stroke beyond 6 hour.2, 3 Practically, as up to 60 % of thrombectomy patients were transferred from a primary stroke center to the comprehensive center for MT, the evaluation of tissues salvageable after delayed MT surgery is important.4 Based on our previous studies showing microstructural change in the infarct region, penumbra, benign oligemia and normal tissue after permanent stroke in rats,5, 6 we hypothesized that the complex reperfusion level in the penumbra after transient middle cerebral artery occlusion (tMCAo) may also be depicted by tensor metrics and further imply the final tissue fate. Our results supported that tensor metrics acquired right before and after recanalization may reflect the survival and reperfusion status in the penumbra after transient stroke.Methods
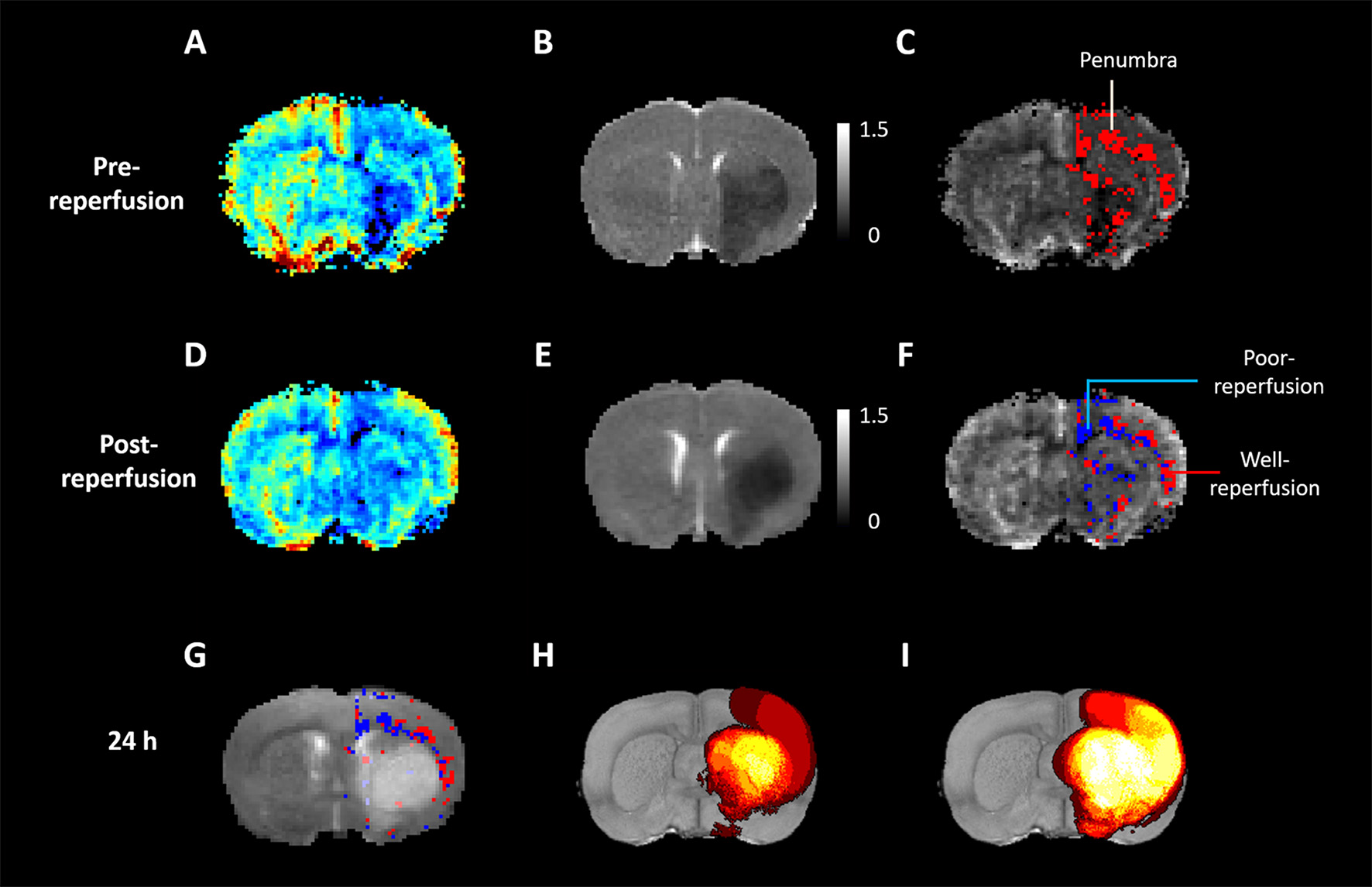
Fourteen Sprague-Dawley rats (n=7 for tMCAo and n=7 for permanent MCAo) were anesthetized with 1-2 % isoflurane following by occlusion of the right middle carotid artery (MCA).6 Briefly, the intra-luminal suture was inserted into the right MCA via external carotid artery thought internal carotid artery. The permanent occlusion was achieved by leaving the suture in the MCA without withdrawal. Multi-parametric MRI including diffusion- and perfusion-MRI, as well as T2w images was performed within 0.5 h and at 3 h after surgery. For tMCAo model, the intraluminal suture was withdrawn within 60 min after occlusion. Multi-parametric MRI was performed in under occlusion and immediately after the suture removal. T2w images at 24 h in both models were acquired to determine the final infarct region. Tensor metrics including fractional anisotropy (FA), apparent diffusion coefficient (ADC), q- and L-value, and relative cerebral blood flow (rCBF) were analyzed as the previous work.5 The reperfusion status of each penumbral pixel was determined by the threshold of 80 % rCBF after suture removal. The tissue survival of each penumbral pixel was defined by the final infarct region delineated by T2w images at 24 h (Fig 1). Tensor metrics in the destined-survival vs. destined-infarct pixels, as well as the well- vs. poor-reperfused pixels at the measurement before and after reperfusion were calculated for statistical comparison. Significant difference between survival or reperfusion status at each time point was assessed using independent t-test (P < 0.05). Significant changes before and after suture removalwere assessed using paired-test (P < 0.05). Error bars were STD.Results & Discussion
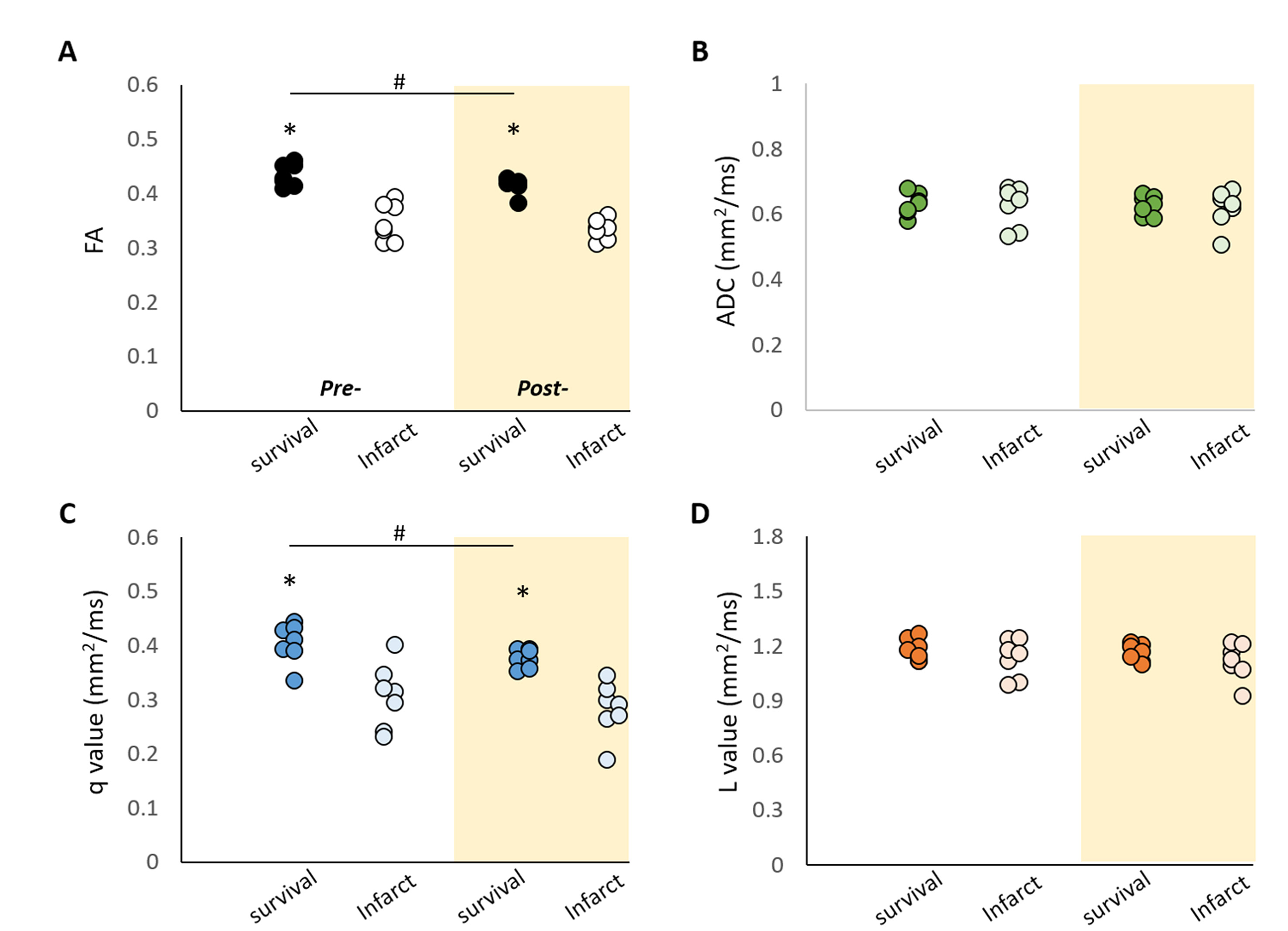
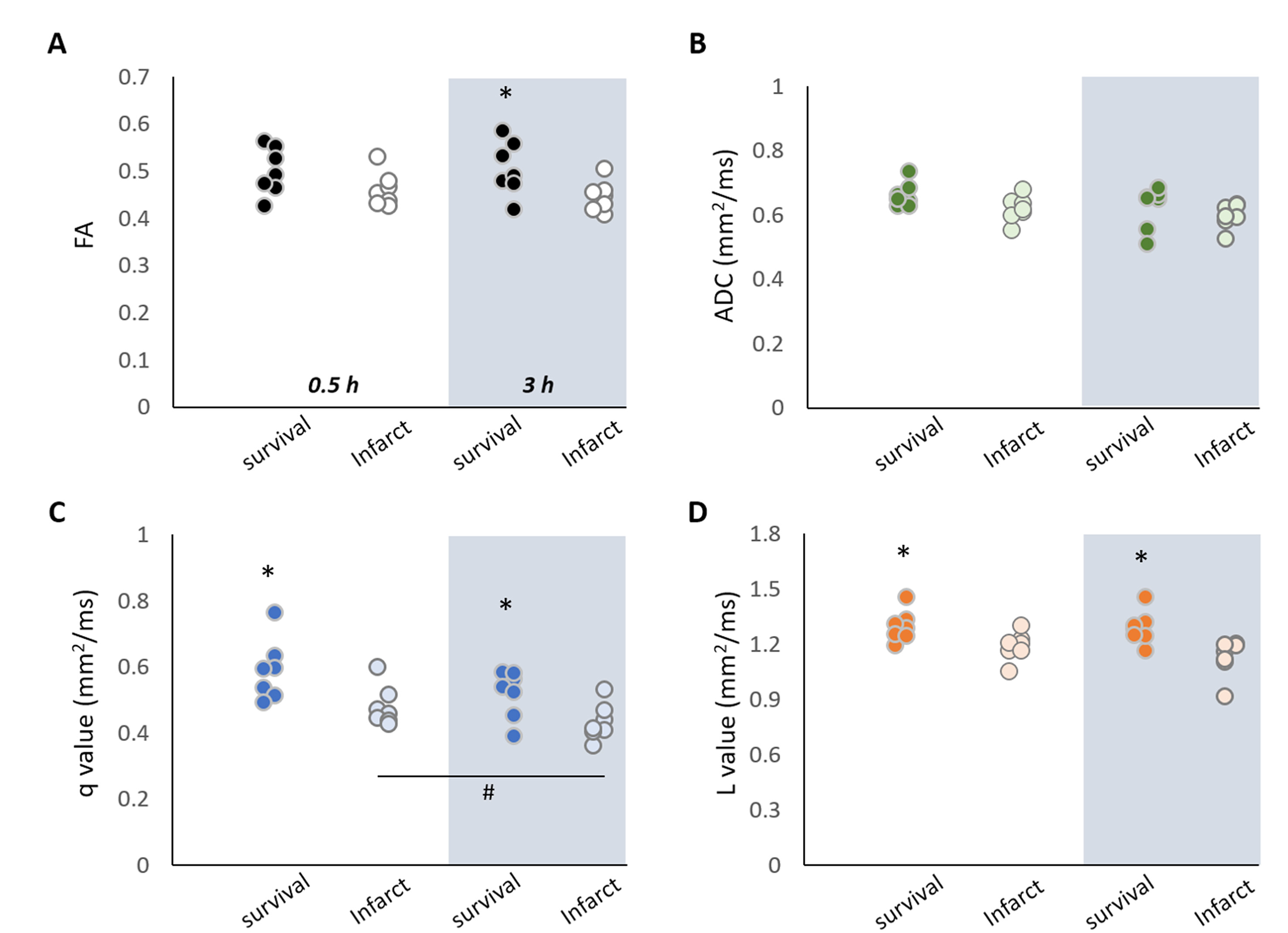
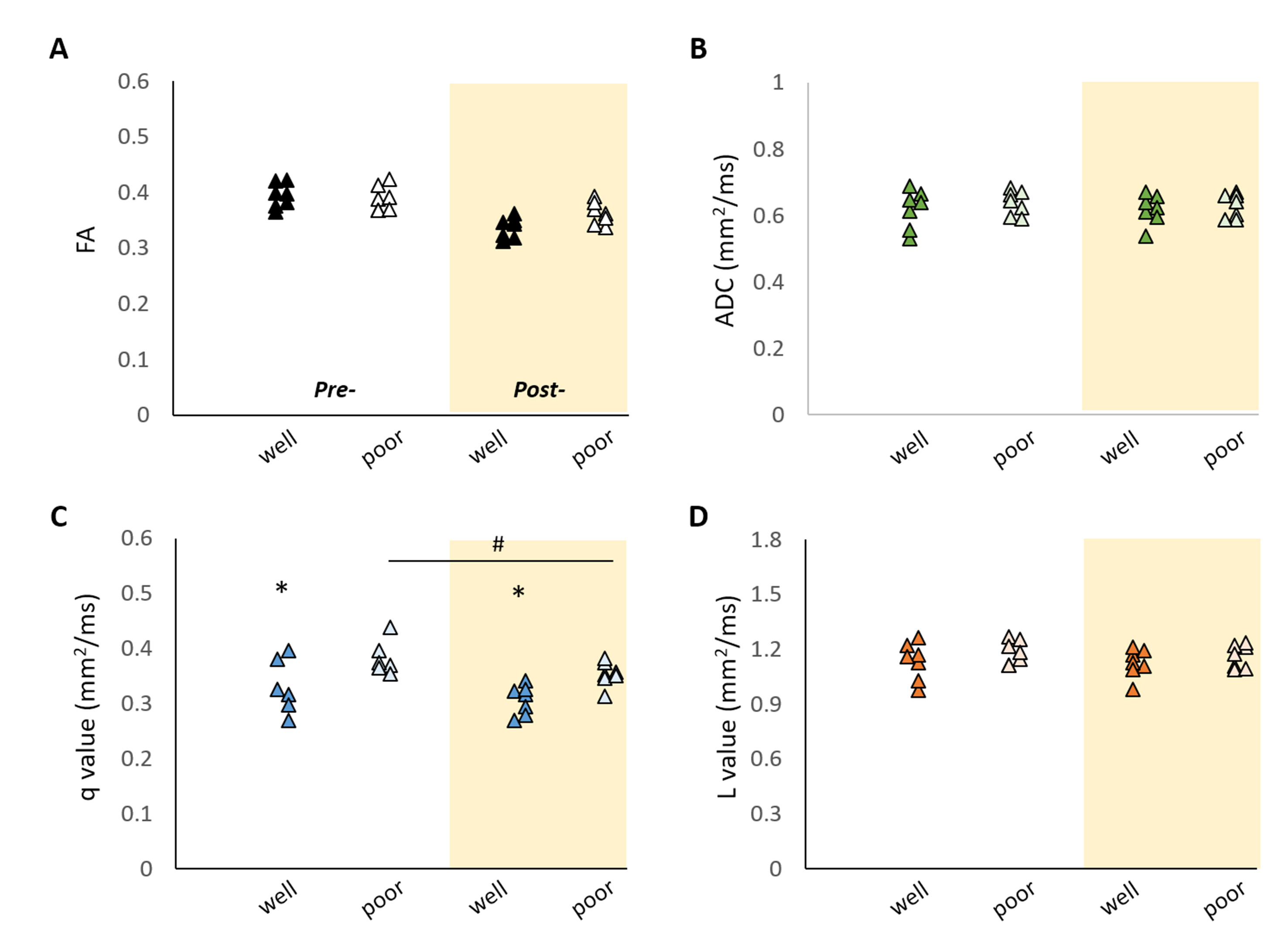
We observed the change of tensor metrics for different survival status in the penumbral tissue after stroke. In tMCAo animals, compared with the destined infarct penumbral tissue, significant higher FA and q-value were observed in destined-survived tissue under occlusion, as well as after suture removal (Fig 2A&C). No significant difference in ADC and L-value was found between survival status in the penumbra (Fig 2B&D). Compared with that after reperfusion, significant higher FA and q-value were observed in destined-survived tissue under occlusion (Fig 2A&C). In pMCAo animals, as significant large final infarct was shown after 24 h (Fig 1I), only a small portion of penumbral tissue (<5%) survived. While no significant difference in FA was found between survival status in the penumbra at 0.5 h in pMCAo animals, higher FA was found at 3 h in the destined survived penumbra tissue (Fig 3A). Significant higher q-value and L-value were observed in destined survived tissue both at 0.5 and 3 h after pMCAo (Fig 3C&D), suggesting microstructural change between the benign oligemia and ischemic penumbra in permanent occlusion.5 Tensor metrics may also describe the reperfusion status in the penumbral tissue after tMCAo (Fig 4). Compared with pixels with poor CBF reperfusion, significant lower q-value was observed in the pixels with well-reperfusion under occlusion and after suture removal (Fig 4C). In addition, pixels with poor reperfusion showed significant lower q-value after reperfusion (Fig 4C). Our results indicate the potential to describe the perfusion status using DTI MRI. Though The paradoxical change of q-value between tissue fate and reperfusion status may indicate the complex reperfusion phenomena among penumbra.7 Our future study will verify the feasibility to predict the tissue fate after tMCAo by the multiple tensor metrics before reperfusion surgery.Acknowledgements
This study was funded in part by Ministry of Science and Technology (MOST 107-2314-B-038-005 and MOST 106-2218-E-039-001-MY3), Taipei, Taiwan.References
1. Powers W J, Rabinstein A A, Ackerson T, et al., 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke, 2018. 49(3): e46-e110.
2. Albers G W, Marks M P, Kemp S, et al., Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N Engl J Med, 2018. 378(8): 708-718.
3. Nogueira R G, Jadhav A P, Haussen D C, et al., Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med, 2018. 378(1): 11-21.
4. Gerschenfeld G, Muresan I P, Blanc R, et al., Two Paradigms for Endovascular Thrombectomy After Intravenous Thrombolysis for Acute Ischemic Stroke. JAMA Neurol, 2017. 74(5): 549-556.
5. Chiu F Y, Kuo D P, Chen Y C, et al., Diffusion Tensor-Derived Properties of Benign Oligemia, True "at Risk" Penumbra, and Infarct Core during the First Three Hours of Stroke Onset: A Rat Model. Korean J Radiol, 2018. 19(6): 1161-1171.
6. Kuo D P, Lu C F, Liou M, et al., Differentiation of the Infarct Core from Ischemic Penumbra within the First 4.5 Hours, Using Diffusion Tensor Imaging-Derived Metrics: A Rat Model. Korean J Radiol, 2017. 18(2): 269-278.
7. del Zoppo G J, Sharp F R, Heiss W D, et al., Heterogeneity in the penumbra. J Cereb Blood Flow Metab, 2011. 31(9): 1836-51.
Figures