3405
Correction of motion artifacts in head and neck diffusion-weighted MRI1Department of Radiation Oncology, Erasmus MC Cancer Institute, Rotterdam, Netherlands, 2Department of Radiology and Nuclear Medicine, Erasmus MC, Rotterdam, Netherlands, 3Department of Medical Informatics, Erasmus MC, Rotterdam, Netherlands
Synopsis
Diffusion-weighted imaging (DWI) is a promising technique for early stratification of responders and non-responders in head and neck chemoradiotherapy. However, data corruption due to swallowing and misalignment reduce the precision of estimated DWI parameters. We investigated different post-processing approaches to improve the reproducibility of the apparent diffusion coefficient (ADC) and demonstrated an improvement in reproducibility from 13.2% to 6.7%. Inter-volume registration showed the largest improvement compared to intra-volume registration and swallowing artifact rejection. The 6.7% reproducibility is sufficient for stratification of responders and non-responders in H&N chemoradiotherapy.
Introduction
Diffusion-weighted imaging (DWI) is a promising technique for response monitoring of head and neck (H&N) carcinomas. However, swallowing and coughing during acquisition can cause signal dropout and can lead to intra- and inter-volume misalignments of the tumor. Both data corruption and misalignment reduce the precision of the estimated DWI parameters and can therefore hamper stratification of responders and non-responders in H&N chemoradiotherapy. The purpose of this study is to identify the most appropriate post-processing methods, including image registration and rejection of corrupted volumes, for intra-voxel incoherent motion (IVIM) DWI.Methods
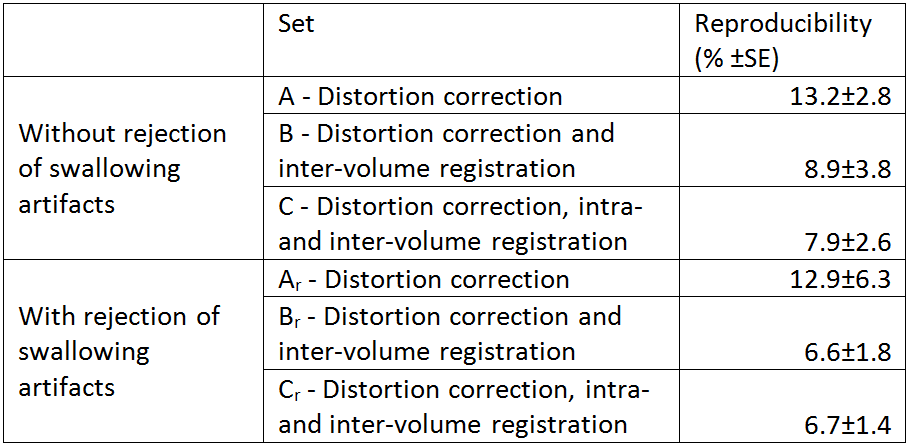
For 5 healthy volunteers two optimized IVIM EPI acquisitions (b-values (repeats): 0(5), 10(7),30(3), 50(1), 60(3), 170(4), 360(2), 830(5), 128x128 matrix, 26x26 cm FOV, ASSET factor 2, 4 mm slice thickness) were obtained in one session on a GE Artist 1.5T scanner (General Electric Medical Systems, Waukesha, WI). During both acquisitions the subjects were asked to swallow at three random points in time. Three different post-processing steps were applied in different combinations: distortion correction only1,2 (set A); distortion correction1,2 and deformable inter-volume registration3 (set B); and distortion correction1,2, deformable intra- and inter-volume registration3 (set C). Next, three additional sets were created by visually detecting and rejecting swallowing artifact corrupted DWI volumes for set A, B and C separately, denoted with subscript r (sets Ar, Br and Cr). This led to a total of 6 post-processed sets per volunteer per acquisition. Subsequently, elliptical ROIs were drawn in both tonsils for each volunteer and IVIM fitting was performed using an in-house fitting script. To determine the optimal post-processing method, the reproducibility of the mean ADC (RADC) in both tonsils was assessed for each set. Reproducibility was defined as the absolute difference in mean ADC between two subsequent acquisitions divided by the mean ADC average over the two acquisitions:
$$R_{adc}=\frac{|\overline{ADC_{1}}-\overline{ADC_{2}}|}{\overline{ADC_{1+2}}}$$
Comparisons between sets A, B and C were performed to assess the influence of registration. Comparisons between sets with and without swallowing artifact rejection were carried out to assess the influence of swallowing artifact rejection.
Results
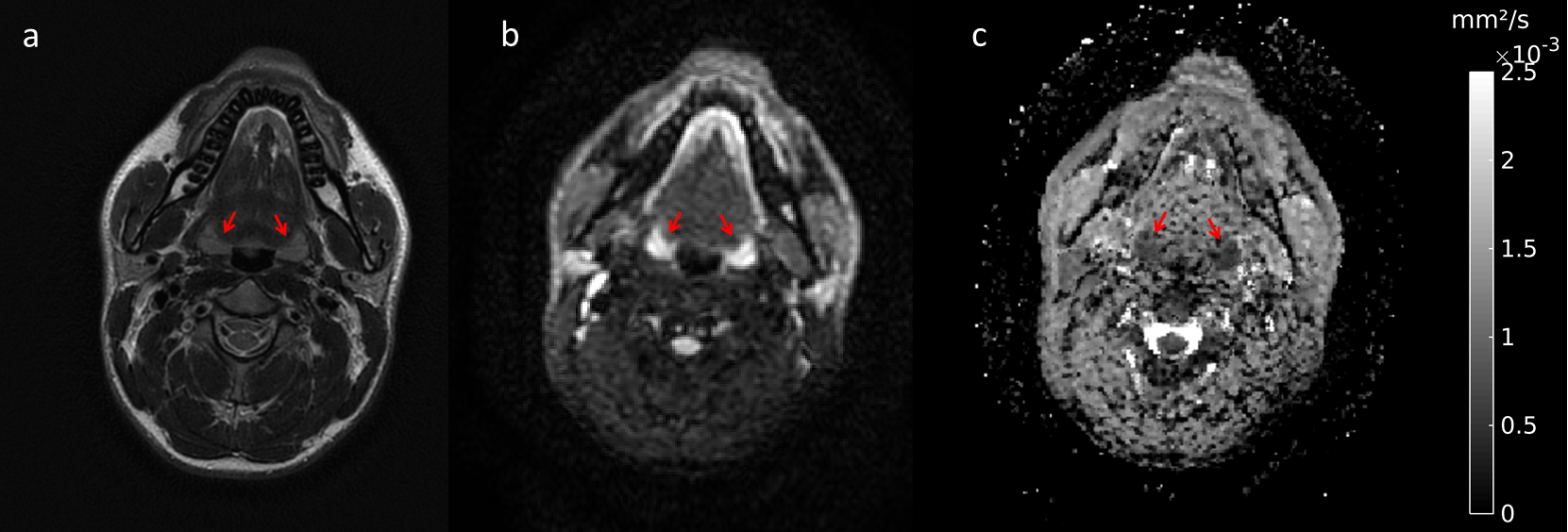
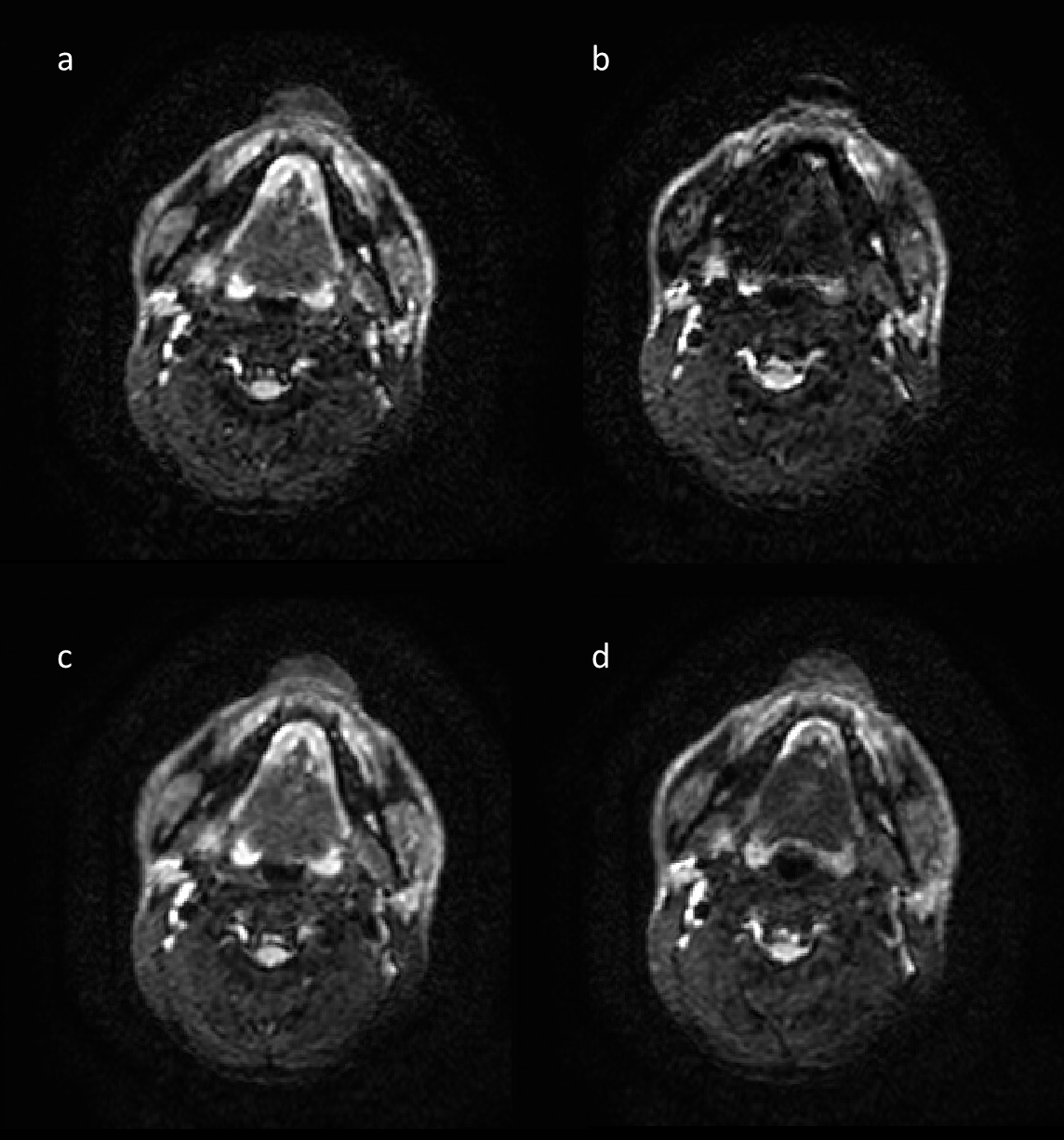
One volunteer was excluded due to severe metal artifacts. Figure 1 shows a slice from a T2-weighted scan and from a b=10 s/mm2 DWI volume as well as the corresponding ADC map of one volunteer from a fully registered acquisition, with the tonsils indicated by red arrows. Table 1 shows an overview of the reproducibility of the mean ADC averaged over the subjects. Reproducibility improved as inter- and intra-volume registration were added. Inter-volume registration led to an improved reproducibility compared to distortion correction alone of 4.3% and 6.3% for cases without and with artifact rejection respectively. Adding intra-volume registration further improved reproducibility by 1% without artifact rejection, but no change was seen in case of artifact rejection. The rejection of swallowing artifacts improved the reproducibility by 2.2% for inter-volume registration and 1.2% for inter- and intra-volume registration. No improvement of artifact rejection was seen for the distortion correction only case. Interestingly, applying intra-volume registration also decreases the severity of swallowing artifacts, as is demonstrated in Figure 2.Discussion
The reproducibility of the mean ADC improved when applying inter-volume or intra- and inter-volume registration. This is in line with expectations, as better aligned data usually results in a more accurate fit result. The effect of swallowing artifact rejection is limited compared to the effect of registration, indicating misalignment is the most dominant source of reduced reproducibility here. Yet, improvement in reproducibility is still seen when applying artifact rejection for both registration cases. The improvement is more pronounced for the inter-volume registration case than for the inter- and intra-volume registration case. This could be due to the fact that intra-volume registration partially compensates swallowing artifacts. However, using intra-volume registration as a way of compensating swallowing artifacts could affect the accuracy of the ADC estimation. Another explanation for the limited effect of swallowing artifact rejection could be that fitting remains relatively robust for swallowing artifacts.Conclusion
Applying inter- and intra-volume registration and swallowing artifact rejection all improved the reproducibility of the mean ADC from an IVIM acquisition from 13.2% to 6.7% on average. Inter-volume registration showed the largest improvement compared to intra-volume registration and swallowing artifact rejection. The achieved reproducibility of the mean ADC after correction is sufficient for stratification of responders and non-responders in H&N chemoradiotherapy.Acknowledgements
No acknowledgement found.References
1. Andersson JL, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. NeuroImage. 2003;20(2):870-888
2. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TEJ, Johansen-Berg H, Bannister PR, De Luca M, Drobnjak I, Flitney DE, Niazy RK, Saunders J, Vickers J, Zhang Y, De Stefano N, Brady JM, Matthews PM. Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage. 2004;23(S1):S208-S219
3. Guyader JM, Bernardin L, Douglas NHM, Poot DHJ, Niessen WJ, Klein S. Influence of image registration on apparent diffusion coefficient images computed from free-breathing diffusion MR images of the abdomen. J Magn Reson Imaging. 2015;42(2):315-330
Figures