3401
Evaluation of an adapted DWI MRI for improved image quality and tissue differentiation in abdominal MRI – a prospective study in oncologic follow-up examinations1Radiology, German Cancer Research Center, Heidelberg, Germany, 2Medical Physics in Radiology, German Cancer Research Center, Heidelberg, Germany, 3Friedrich-Alexander University Erlangen-Nürnberg, Erlangen, Germany, 4Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Diffusion-Weighted imaging is a mainstay for oncologic examinations. However, abdominal examinations with standard DWI can be challenged by signal exploration and motion artifacts. This prospective study therefore compares a standard EPI-DWI with an oncologically optimized-DWI, including complex averaging, motion correction between averages, rescaling of motion corrupted averages, and background suppression, in oncological follow-up MRI investigations. A diffusion resolution phantom demonstrated an improved image quality by the optimized-DWI. Image quality analysis of prospectively acquired abdominal DWI MRI examinations in 52 patients showed a significant improvement in image quality and apparent signal-to-background-noise-ratio by optimized-DWI as compared to standard EPI-DWI in oncologic imaging.
Introduction
Diffusion-Weighted imaging (DWI) is an important part of oncological magnetic resonance imaging (MRI). However, abdominal studies can be challenged by motion artifacts, poor signal-to-noise-ratios (SNR) and visibility of retroperitoneal structures, which is why it needs to be improved depending on the investigated region[1]. This study aims at prospectively evaluating an oncologically adapted DWI sequence for improved image quality and tissue differentiation in patients with abdominal malignancies.Methods
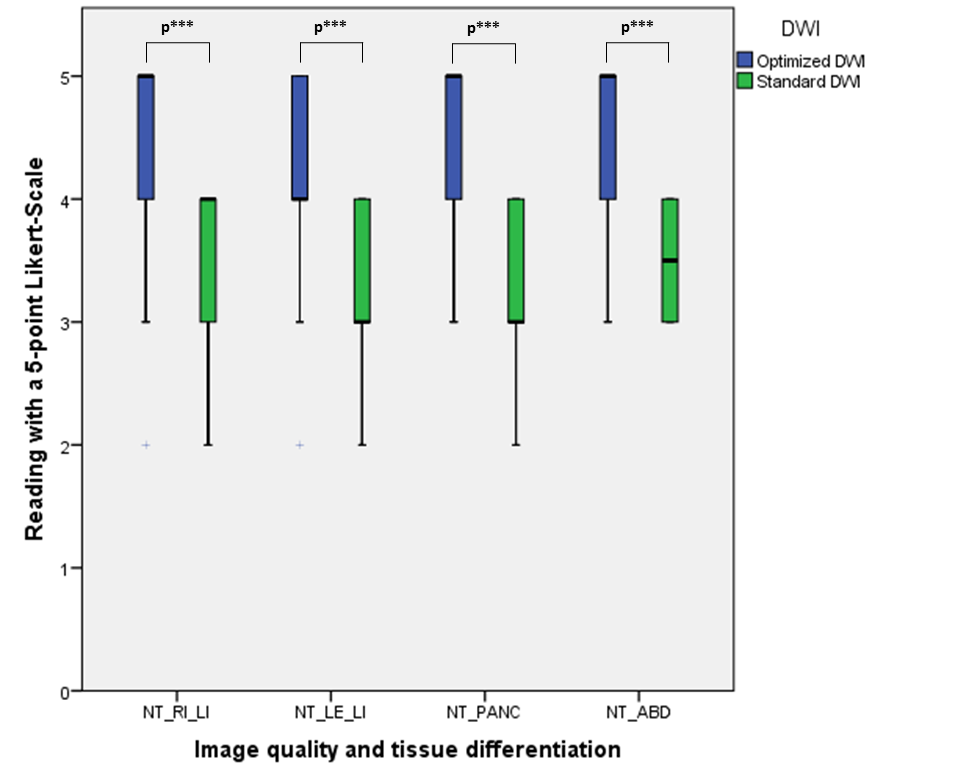
This IRB-approved, prospective in-vivo and ex-vivo study included phantom measurements and oncological patient examinations of the abdomen. For the phantom experiments, a diffusion resolution phantom was used with chambers of triangular cross section containing aqueous polyvinylpyrrolidone (PVP-K30) solution with alternating concentration and thus different diffusion-coefficients (10%w/w and 43%w/w corresponding to D=1.6µm²/ms and D=0.5µm²/ms). 52 prospectively acquired oncologic abdominal MRI examinations (mean age: 57years; male/female: 21/31) using a 1.5T MRI scanner (MAGNETOM Aera, Siemens Healthcare GmbH, Germany) included both a standard-EPI-DWI (“s-DWI”; b=50,900s/mm²) and an oncologically adapted, prototype optimized-DWI (“opt-DWI”; EPI-DWI with b=0,50,900,1500s/mm² and advanced processing, including complex averaging, motion correction between the averages, rescaling of motion corrupted averages, and background suppression). The following parameters were used for s-DWI: TR=6.5s; TE=63ms; FOV 450x242mm²; matrix 134x72; resolution 3.4x3.4mm², interpolated to 1.7x1.7mm²; slice thickness 5mm; bandwidth 2332Hz/Px; b-values 50,900s/mm² (2,8 averages), gradient mode 3-scan trace, 90 slices in 3 steps, 11min. For opt-DWI: TR=7.9s; TE=57ms; FOV 480x270mm²; matrix 164x92; resolution 3x3mm², interpolated to 1.5x1.5mm²; slice thickness 5mm; bandwidth 2540Hz/Px; b-values 0,50,900,1500s/mm² (1,1,16,18 averages); gradient mode 3D-diagonal; 90 slices in 3 steps, 15min. At the setting of b=900s/mm², apparent-ratio of signal intensity in the normal tissue/standard deviation in the non-background-suppressed surrounding air was quantitatively evaluated, image quality and tissue differentiation parameters were rated by two independent, blinded readers using a 5-point Likert-Scale[2]. Statistics included Wilcoxon-signed-rank-test and kappa-statistic (p<0.05).Results
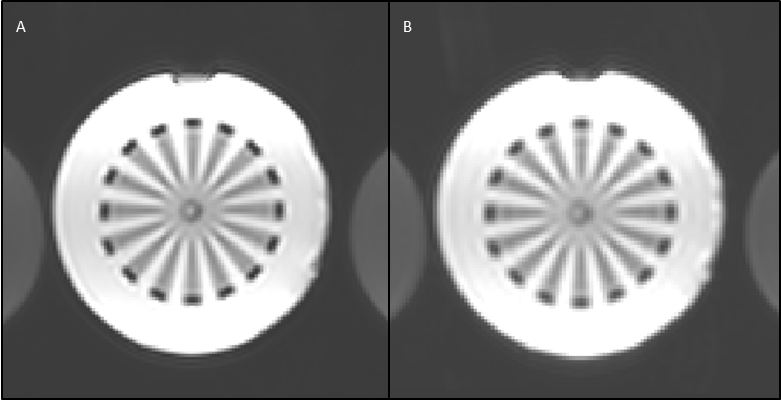
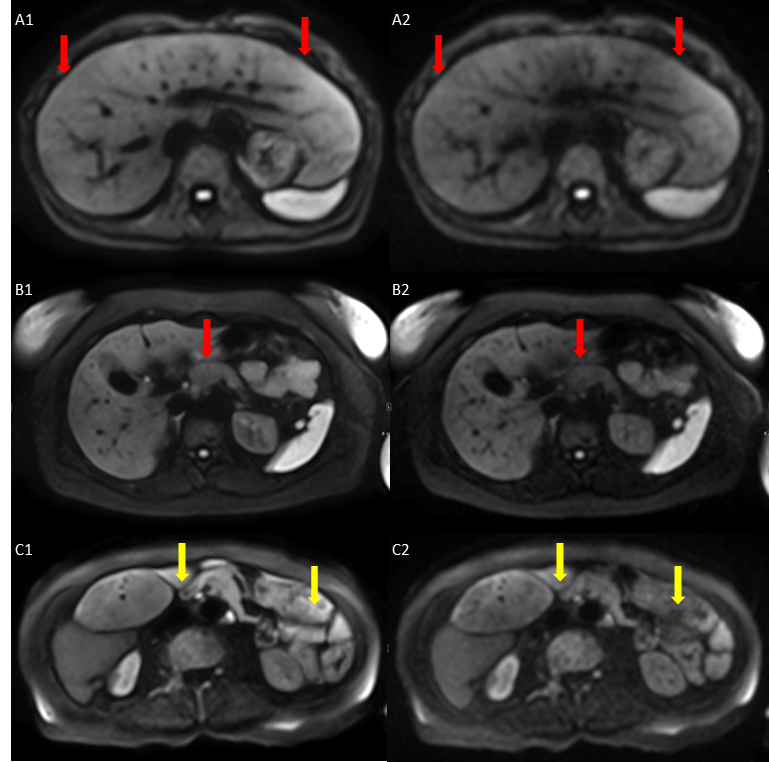
The DWI-phantom demonstrated an optimized contour sharpness and inlay differentiation for the opt-DWI (Figure 1). The apparent-ratio of the signal intensity of normal tissue/standard deviation of non-background-suppressed surrounding air of b900-DWI of the right/left hemiabdomen was significantly increased in opt-DWI (mean: 227±250/150±192) vs. s-DWI (mean: 37±17/40±23) (p<0.001). Image quality parameters (contour sharpness right/left liver and pancreas) were significantly increased in opt-DWI vs. s-DWI (p<0.001) (Figure 2,3). Central parts of the abdomen had decreased shading effects in opt-DWI vs. s-DWI (Figure 3). Tissue differentiation for the upper abdominal and retroperitoneal structures was significantly increased in opt-DWI vs. s-DWI (p<0.001) (Figure 2). Interreader reliability test showed good agreement (kappa=0.754) (p<0.001).Discussion
This study prospectively evaluated an oncologically adapted DWI by ex-vivo phantom measurements and in-vivo oncological follow-up MRI examinations. The superiority of the optimized prototype DWI, including improved image resolution, motion correction between the averages, background suppression and decreased shading effects by rescaling of motion corrupted averages, could be demonstrated. Oncological DWI optimization should be performed to improve screening and follow-up examinations[3], possibly leading to an advanced patient care.Conclusion
This prospective study demonstrates the superiority of an oncologically optimized DWI with an improved image resolution, motion correction between the averages and background suppression over standard EPI-DWI for abdominal oncological imaging. Assessment of anatomical structures including the retroperitoneum was significantly improved using the novel approach in oncological follow-ups.Acknowledgements
Special acknowledgments and thanks to Siemens Healthineers for providing the optimized prototype sequence and protocol that did build the basis of the further adapted sequence.References
1. Taron, J., et al., Clinical Robustness of Accelerated and Optimized Abdominal Diffusion-Weighted Imaging. Invest Radiol, 2017. 52(10): p. 590-595.
2. de Winter, J.C.F., Dodou, D., Five-point Likert items: T test versus Mann–Whitney–Wilcoxon. Practical Assessment, Research & Evaluation, 2010. 15(11): p. 16.
3. Zhang, T.T., et al., Differentiation of pancreatic carcinoma and mass-forming focal pancreatitis: qualitative and quantitative assessment by dynamic contrast-enhanced MRI combined with diffusion-weighted imaging. Oncotarget, 2017. 8(1): p. 1744-1759.
Figures