3357
Acquisition and processing strategy for obtaining high quality, distortion free diffusion MRI of the brainstem and cervical spine1Quantitative Medical Imaging Section, National Institute of Biomedical Imaging and Bioengineering, NIH, Bethesda, MD, United States, 2NIH MRI Research Facility, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD, United States, 3Laboratory of Brain and Cognition, National Institute of Mental Health, NIH, Bethesda, MD, United States, 4Medical Genomics and Metabolic Genetics Branch, National Human Genome Research Institute, NIH, Bethesda, MD, United States, 5Henry M. Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD, United States, 6NIH, Bethesda, MD, United States, 7Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 8Icahn School of Medicine at Mount Sinai, New York City, NY, United States
Synopsis
Despite its clear clinical and research usefulness, high quality in-vivo diffusion MRI imaging of the brainstem and the cervical spine has been challenging due to susceptibility-induced distortions and ghosting in echo planar images (EPI). In this study, we propose an acquisition and data processing strategy that can be carried out on clinical scanners with commonly available EPI sequences with good resolution and in a reasonable scan time (less than 30 minutes). We apply this acquisition strategy to the study of pyramidal decussation in subjects with Moebius syndrome and mirror movements.
Introduction
Despite its clear clinical and research usefulness, high quality in-vivo diffusion MRI imaging of the brainstem and the cervical spine has been challenging due to susceptibility-induced distortions and ghosting in echo planar images (EPI). In this study, we propose an acquisition and data processing strategy that can be carried out on clinical scanners with commonly available EPI sequences with good resolution and in a reasonable scan time (less than 30 minutes). Our approach entails acquiring DWIs in multiple planes, each with different phase encoding direction (PE), and processing all data together to obtain a final diffusion tensor (DT) dataset with correct morphology and more immune from ghosting artifacts. We apply this method to a group of healthy controls and subjects with Moebius syndrome1,2,3 (MBS) and mirror movements4. Mirror movements are defined as simultaneous contralateral involuntary movement of one side of the body that accompany similar voluntary movement of the opposite side4. A possible mechanism contributing to mirror movements could be an abnormal decussation of the descending corticospinal motor tracts (CST) in the medulla oblongata. We assess if the high quality DTI data would detect differences in CST decussation between patients and controls.Methods
All participants were scanned on a GE system with head-neck-spine
coil. A total of 180 DWI volumes were collected for each subject.
Given the shape of the brainstem and cervical spine,
data were collected in both sagittal and coronal planes to reduce the number of
slices that need to be acquired. This enables us to address ghosting
artifacts that might be present in one plane, but not the other. To
correct for EPI induced distortions, the acquisition was repeated with four PEs,
AP and PA for sagittal data, and LR and RL for coronal data. For each PE, 45 volumes with maximum b-value of 900 s/mm2 were
collected. T2W scans were also acquired in both sagittal and coronal planes
with a fast spin echo sequence. Data were processed using TORTOISE5 to
correct for motion and eddy current distortions6. EPI
distortion correction was done in three steps: 1) Sagittal data were merged
into one corrected dataset using the estimated deformation fields from opposite
PEs (AP/PA) and information from T2WIs using DR-BUDDI7. The
diffusion tensor (DT) was computed for the corrected DWIs using the weighted
least square tensor estimation. 2) Coronal data (RL/LR PEs) were
merged into one corrected dataset in a similar manner as AP/PA. 3) Tensor-based DR-TAMAS8
registration was used to create a subject specific DT template from DTAP/PA
and DTRL/LR.
Control subjects’ DTs were used to create a study-specific control template
using DR-TAMAS, and subsequently all subjects’ DTs were registered to this template. Directionally encoded color maps (DEC maps)9
were created for each subject. Four healthy volunteers (mean age: 27.5 years)
with no history of neurological disorders and normal MRI, and two subjects (18
and 53 years) diagnosed with MBS and mirror movements are included
here.
Results
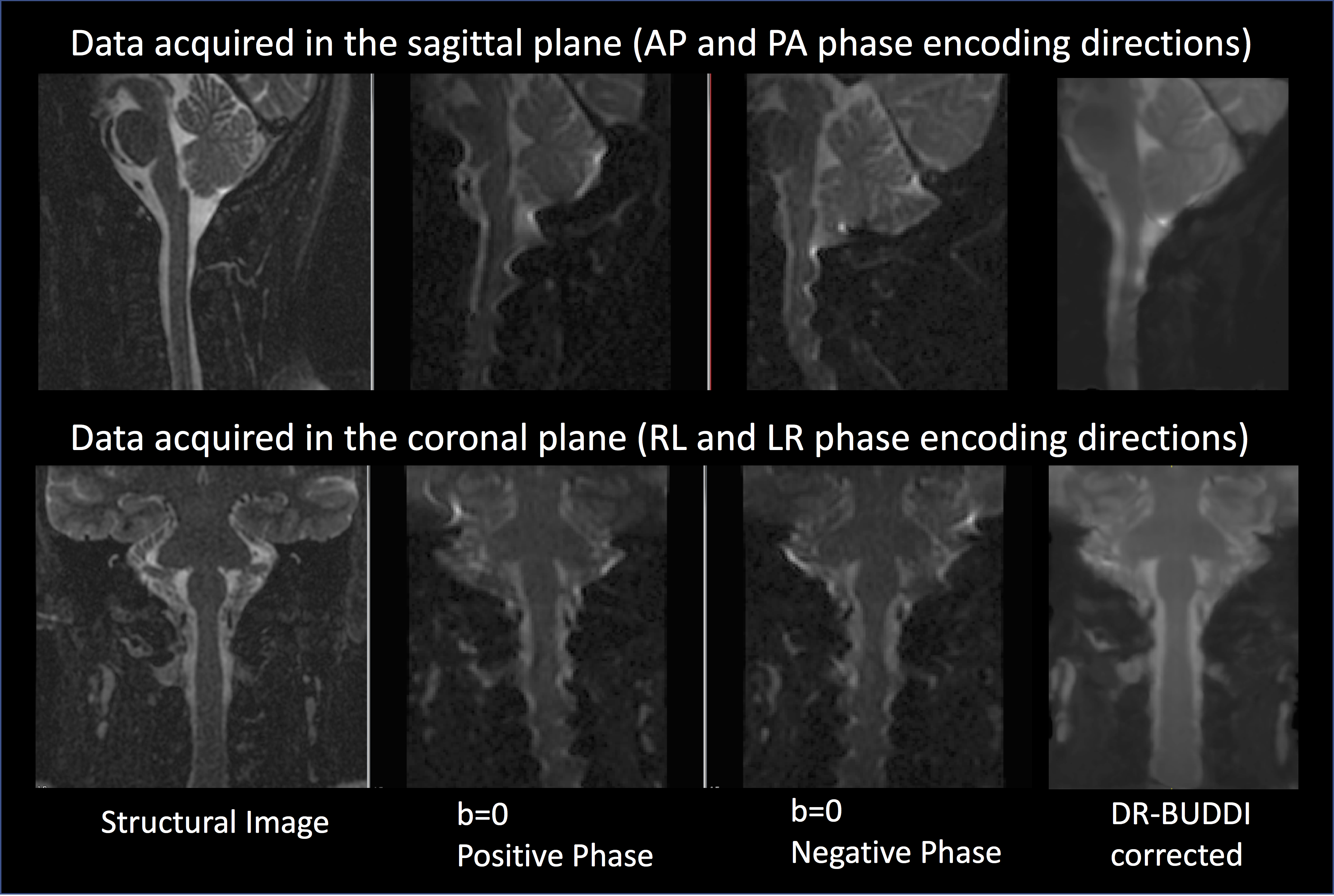
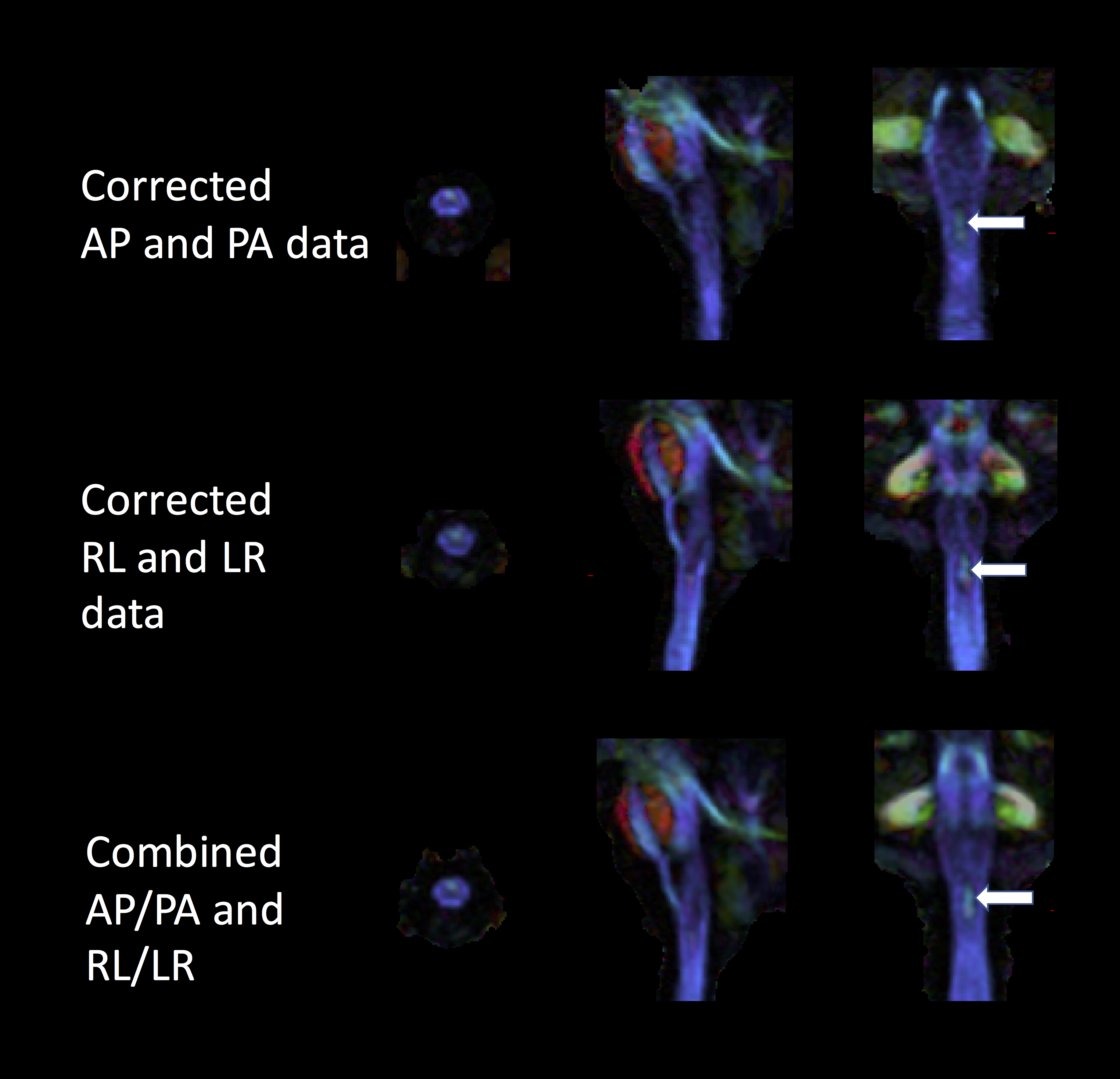
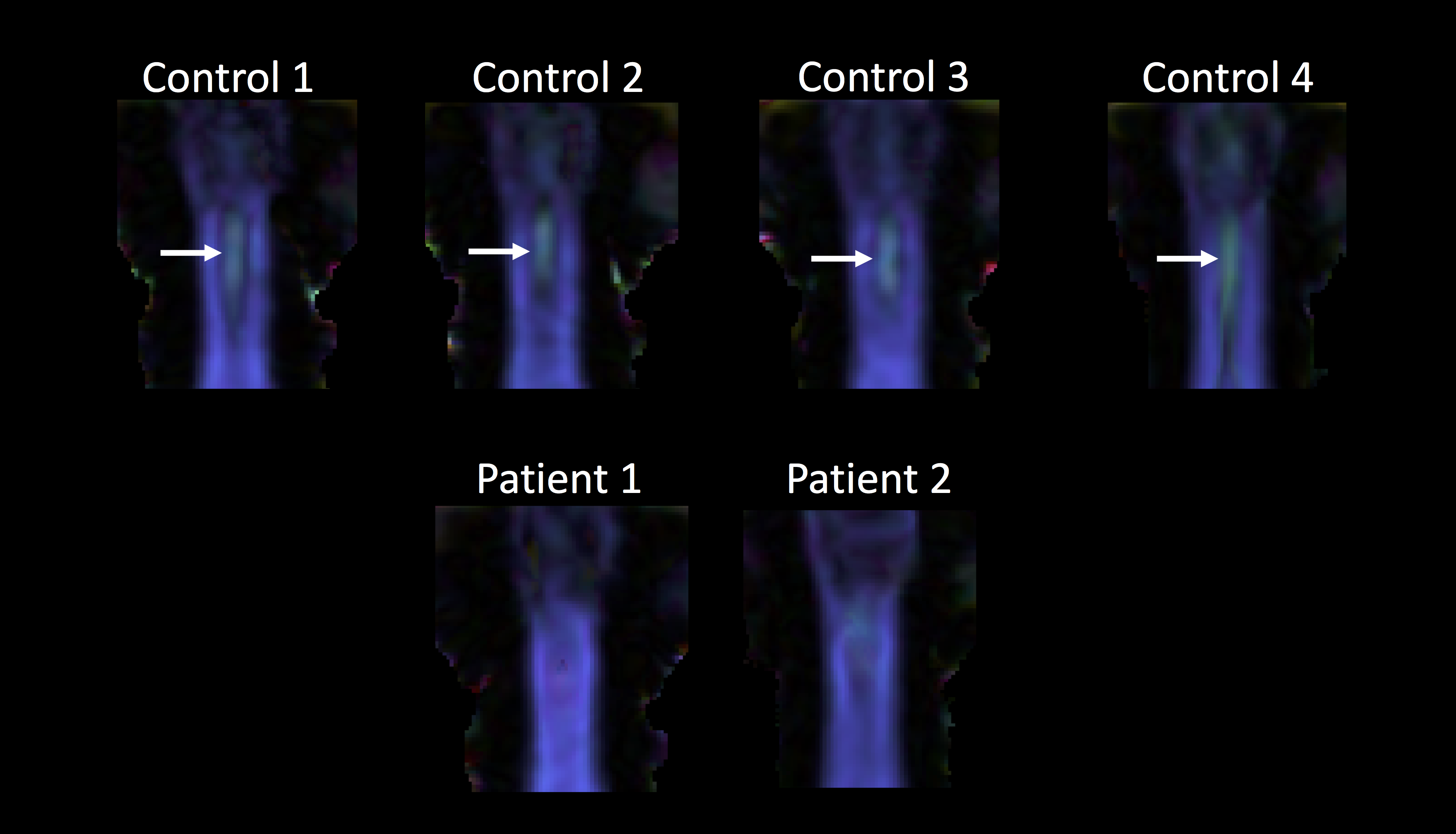
Figure 1 displays the original distorted and the corresponding corrected b=0 s/mm2 images after correction for EPI distortions for data acquired in sagittal and coronal planes of a single subject. The corrected b=0 images clearly show that the EPI distortions are significantly reduced and match more closely to the T2W structural image. Figure 2 displays the DEC map computed from DR-BUDDI corrected sagittal (AP/PA) and coronal (RL/LR) data along with the combined (AP/PA and RL/LR) data at the bottom. The decussation of pyramids is visible in all three; however, it is more well defined in the combined dataset as it has a higher SNR. Figure 3 shows the images for all the controls and patients with mirror movements. Decussation of pyramids is clearly visible for all the control subjects but missing or not observable for the subjects with Moebius syndrome and mirror movements.Discussion
Acquiring multiple slice planes and PEs provides the EPI distortion algorithms with additional information and constraints, regularizing the registration and making it more robust to artifacts. We presented a successful application of this acquisition and processing strategy in detecting differences in CST decussation between patients and controls. This strategy proves useful for imaging the brainstem and the cervical spine and can be applied to study other disorders. In clinical settings where the scan time is limited, many favor acquiring more DWI directions with a single PE, rather than acquiring different PEs and additional slice planes. However, the latter approach is advantageous as it enables post-processing correction of many distortion and ghosting artifacts. In this study, we used the same gradient table for all four PEs, however, one can increase the number of directions by using different sets for AP/PA and RL/LR, taking advantage of both strategies.Acknowledgements
We would like to thank the research participants. Support for this work is provided by U01 HD079068-03 and a Moebius Syndrome Foundation research grant.References
1. Möbius P.J. Ueber angeborene doppelseitige Abducens-Facialis- Lahmung. MMW Munch Med Wochenschr 1888;35:91–4.
2. Möbius, P.J., 2008. About congenital bilateral abducens and facialis palsy. Strabismus, 16(1), pp.39-44.
3. Verzijl, H.T., van der Zwaag, B., Cruysberg, J.R. and Padberg, G.W., 2003. Möbius syndrome redefined A syndrome of rhombencephalic maldevelopment. Neurology, 61(3), pp.327-333.
4. Webb, B., Frempong, T., Naidich, T.P., Gasser, H., Jabs, E.W., Rucker, J.C., 2014. Mirror movements identified in patients with Moebius syndrome. Tremor Other Hyperkinet Mov (NY). Jul 22 (4), pp. 256.
5. Pierpaoli, C., Walker, L., Irfanoglu, M., Barnett, A., Chang, L.-C., Koay, C., Pajevic, S., Rohde, G., Sarlls, J. and Wu, M., 2010. TORTOISE: an integrated software package for processing of diffusion MRI data. ISMRM 19th annual meeting, Stockholm, Sweden.
6. Rohde, G. K., Barnett, A. S., Basser, P. J., Marenco, S. and Pierpaoli, C., 2004. Comprehensive approach for correction of motion and distortion in diffusion-weighted MRI. Magn Reson Med 51(1), pp.103–114.
7. Irfanoglu, M.O., Modi, P., Nayak, A., Hutchinson, E.B., Sarlls, J. and Pierpaoli, C., 2015. DR-BUDDI (Diffeomorphic Registration for Blip-Up Blip-Down Diffusion Imaging) method for correcting echo planar imaging distortions. NeuroImage, 106, pp.284-299.
8. Irfanoglu, M. O., Nayak, A., Jenkins, J., Hutchinson, E., Sadeghi, N., Thomas, C. and Pierpaoli, C., 2016. DR-TAMAS: Diffeomorphic registration for tensor accurate alignment of anatomical structures. NeuroImage 132, pp. 439–454.
9. Pajevic, S., Pierpaoli, C., 1999. Color schemes to represent the orientation of anisotropic tissues from diffusion tensor data: application to white matter fiber tract mapping in the human brain. Magn. Reson. Med. 42, 526–540.
Figures