3332
Multimodal Models Provide Earlier Prediction (10 Years Prior to Diagnosis) of Dementia and Cognitive Decline and Personalized Actionability for Risk Mitigation for At-Risk Individuals1Human Longevity, Inc., San Diego, CA, United States, 2Electrical and Computer Engineering, University of Illinois at Urbana-Champaign, Urbana, IL, United States
Synopsis
Current approaches for predicting an individual’s risk of developing dementia rely primarily on single modality data and/or single biomarkers. Here we evaluate the utilization of non-invasive MR imaging and genetics for early detection and prediction of cognitive decline and dementia. We demonstrate
Introduction
Dementia is a leading cause of disability globally, affecting 5-7% of people over 60 years old1. Many at-risk will outlive the onset of the disease progression2. According to recent analyses, 28-35% of an individual’s lifetime risk is potentially modifiable3. To facilitate intervention, disease needs to be detected and identified as early as possible; biomarkers need to be measurable 5-10 years prior to the onset of clinically diagnosable disease.
Current approaches for predicting dementia risk rely primarily on single modality data and/or single biomarkers. For example, APOE status is a well-documented genetic biomarker for risk of developing Alzheimer’s disease4,5. Polygenic hazard scores (PHS) have also been published, but are not widely used in clinical practice6. Similarly, hippocampal occupancy score (HOC) is used to detect onset of dementia7,8. The current gold standard for Alzheimer’s detection is amyloid PET9, however, it is costly and invasive.
Beyond inherited risk, strong evidence exists for causal associations between certain modifiable risk factors and developing dementia. Recommendations include reduction of tobacco use10 and better control of hypertension11,12. Other modifiable factors include alcohol use13,14, sleep, management of diabetes, BMI15–17, and plasma homocysteine18–21, plasma vitamin B1218–21, plasma albumin levels22–24, and triglyceride levels25. Although risk models for progression from mild cognitive impairment to dementia exist26, no one has combined such a model with early detection and actionability. Moreover, others have not yet compared the performance of such an approach to amyloid PET. We present a method for early detection of cognitive decline using non-invasive imaging and genetics joined with a model that identifies potentially modifiable factors upon which an individual can act to mitigate their risk.
Methods
Multimodal inputs to our models comprise a PHS calculated from known, common genetic markers associated with Alzheimer’s disease27, quantitative morphometric values derived from segmented structural MRIs of the brain, and modifiable factors indicated in the medical literature to influence an individual’s risk of developing dementia7-22.
A number of machine learning models were trained using ADNI data and validated with NACC data to assess the diagnostic status and predict cognitive decline in individuals using their genetic and imaging markers. A Cox proportional hazards (CPH) model was trained to predict the time the onset of dementia, using MRI data from up to 10 years prior to onset. The trained model computes a relative risk for each individual, which is combined with epidemiologic data to determine the absolute age-adjusted risk.
Finally, we develop a framework built on observational data28 from ADNI and NACC. This approach incorporates in silico experimentation to evaluate the conditional average treatment effect (CATE) for an individual after changing specific modifiable risk factors. We leverage this information to develop a personalized action plan.
Results
Our multimodal prediction model utilizing MRI features and a PRS better predicts a diagnosis of mild cognitive impairment (MCI) or dementia than APOE status or HOC (Figure 1a). It also performs better than cognitive testing (Figure 1b).
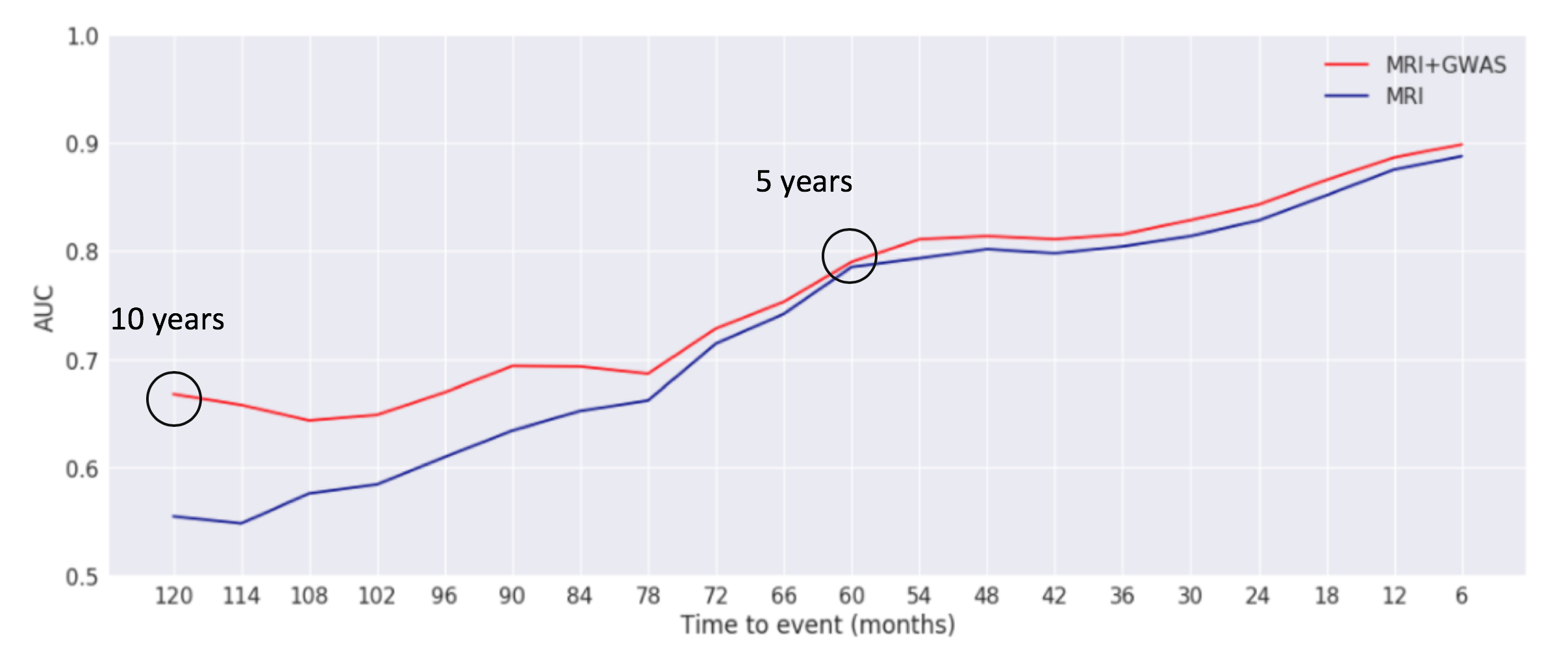
The combination of genetics and MRI features allows for improved prediction 10 years prior to the diagnosis of dementia than MRI features alone (Figure 2).
Our MRI plus genetics model has equivalent performance to amyloid PET 10 years prior to diagnosis and is more accurate in predicting onset of dementia closer to the time of the event (Figure 3a). In addition, our model is better able to distinguish among normal, MCI and dementia that amyloid PET (Figure 3b&c).
We have developed a personalized recommendation system that allows for high-risk individuals to evaluate the impact of mitigating modifiable risk factors to reduce their short-term risk of disease progression (Figure 4). An example of one individual is shown, illustrating the absolute age-adjusted risk of dementia derived from the relative risk from the survival model and epidemiologic data, as well as the personalized action plan developed from the risk mitigation framework.
Multiple models were evaluated and a recurrent neural network was found to perform the best (Figure 5).
Discussion/Conclusion
We demonstrate that prediction models for the onset of MCI and dementia benefit from the integration of multiple modalities and show that incorporation of multiple features within each modality (i.e. multiple genetic markers and multiple neuroanatomical features) further enhances the predictive value of models. In the future, incorporating the remaining 13,000 samples available in additional cohorts (e.g. UK Biobank) with our automated method described in Wu et al29 will further improve our models. Our non-invasive method compares favorably with amyloid-PET, and we illustrate that our approach provides actionability for risk information, allowing high-risk individuals to evaluate how they might mitigate their risk of disease progression using modifiable risk factors.Acknowledgements
No acknowledgement found.References
- Schwarzinger M, Pollock BG, Hasan OSM, et al. Contribution of alcohol use disorders to the burden of dementia in France 2008–13: a nationwide retrospective cohort study. Lancet Public Heal. 2018. doi:10.1016/S2468-2667(18)30022-7
- Baumgart M, Snyder HM, Carrillo MC, Fazio S, Kim H, Johns H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s Dement. 2015;11(6):718-726. doi:10.1016/j.jalz.2015.05.016
- Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673-2734. doi:10.1016/S0140-6736(17)31363-6
- Myers RH, Schaefer EJ, Wilson PW, et al. Apolipoprotein E epsilon4 association with dementia in a population-based study: The Framingham study. Neurology. 1996. doi:10.1212/WNL.46.3.673
- Saunders AM, Strittmatter WJ, Schmechel D, et al. Association of apolipoprotein E allele ϵ4 with late-onset familial and sporadic alzheimer’s disease. Neurology. 1993.
- Desikan RS, Schork AJ, Wang Y, et al. Polygenic Overlap Between C-Reactive Protein, Plasma Lipids, and Alzheimer Disease. Circulation. 2015. doi:10.1161/CIRCULATIONAHA.115.015489
- McEvoy L, Brewer J. Biomarkers for the clinical evaluation of the cognitively impaired elderly: amyloid is not enough. Imaging Med. 2012. doi:10.2217/iim.12.27.Biomarkers
- Heister D, Brewer JB, Magda S, Blennow K, McEvoy LK. Predicting MCI outcome with clinically available MRI and CSF biomarkers. Neurology. 2011. doi:10.1212/WNL.0b013e3182343314
- Iaccarino L, Chiotis K, Alongi P, et al. A Cross-Validation of FDG-and Amyloid-PET Biomarkers in Mild Cognitive Impairment for the Risk Prediction to Dementia due to Alzheimer’s Disease in a Clinical Setting. J Alzheimer’s Dis. 2017;59(2):603-614. doi:10.3233/JAD-170158
- Peters R, Peters J, Warner J, Beckett N, Bulpitt C. Alcohol, dementia and cognitive decline in the elderly: A systematic review. Age Ageing. 2008;37(5):505-512. doi:10.1093/ageing/afn095
- Qui C, Strauss E Von, Fastbom J, Winblad B, L. Low blood pressure and risk of dementia in the Kungsholmen project. Arch Neurol. 2003.
- Jochemsen HM, Muller M, Visseren FL, et al. Blood pressure and progression of brain atrophy the SMART-MR study. JAMA Neurol. 2013. doi:10.1001/jamaneurol.2013.217
- Heymann D, Stern Y, Cosentino S, Tatarina-Nulman O, Dorrejo JN, Gu Y. The Association Between Alcohol Use and the Progression of Alzheimer’s Disease. Curr Alzheimer Res. 2016. doi:10.2174/1567205013666160603005035
- Gu Y, Scarmeas N, Short EE, et al. Alcohol intake and brain structure in a multiethnic elderly cohort. Clin Nutr. 2014. doi:10.1016/j.clnu.2013.08.004
- Blondell SJ, Hammersley-Mather R, Veerman JL. Does physical activity prevent cognitive decline and dementia?: A systematic review and meta-analysis of longitudinal studies. BMC Public Health. 2014. doi:10.1186/1471-2458-14-510
- Guure CB, Ibrahim NA, Adam MB, Said SM. Impact of Physical Activity on Cognitive Decline, Dementia, and Its Subtypes: Meta-Analysis of Prospective Studies. Biomed Res Int. 2017. doi:10.1155/2017/9016924
- Liu R, Sui X, Laditka JN, et al. Cardiorespiratory fitness as a predictor of dementia mortality in men and women. Med Sci Sports Exerc. 2012. doi:10.1249/MSS.0b013e31822cf717
- Shen L, Ji H-F. Associations between Homocysteine, Folic Acid, Vitamin B12 and Alzheimer’s Disease: Insights from Meta-Analyses. J Alzheimers Dis. 2015. doi:10.3233/JAD-150140
- Li M-M, Yu J-T, Wang H-F, et al. Efficacy of vitamins B supplementation on mild cognitive impairment and Alzheimer’s disease: A systematic review and meta-analysis. Curr Alzheimer Res. 2014.
- Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: Systematic review and meta-analysis. BMC Public Health. 2014. doi:10.1186/1471-2458-14-643
- Gröber U, Kisters K, Schmidt J. Neuroenhancement with Vitamin B12-underestimated neurological significance. Nutrients. 2013. doi:10.3390/nu5125031
- Kim T-S, Pae C-U, Yoon S-J, et al. Decreased plasma antioxidants in patients with Alzheimer’s disease. Int J Geriatr Psychiatry. 2006. doi:10.1002/gps.1469
- Llewellyn DJ, Langa KM, Friedland RP, Lang I a. Serum albumin concentration and cognitive impairment. Curr Alzheimer Res. 2010. doi:10.2174/1872209197471563128
- Maes M, Devos N, Wauters A, et al. Inflammatory markers in younger vs elderly normal volunteers and in patients with Alzheimer’s disease. J Psychiatr Res. 1999. doi:10.1016/S0022-3956(99)00016-3
- Burgess B, McIsaac S, Naus K, Chan J. Elevated plasma triglyceride levels precede amyloid deposition in Alzheimer’s disease mouse models with abundant Aβ in plasma. Neurobiol Dis. 2006. doi:10.1016/j.nbd.2006.06.007
- Kauppi K, Fan CC, McEvoy LK, et al. Combining polygenic hazard score with volumetric MRI and cognitive measures improves prediction of progression from mild cognitive impairment to Alzheimer’s disease. Front Neurosci. 2018;12(APR):1-7. doi:10.3389/fnins.2018.00260
- Lambert J-C, Ibrahim-Verbaas C, Harold D, et al. Meta-analysis of 74,046 individuals indetifies 11 new susceptibility loci for Alzheimer’s disease. Nat Genet. 2014. doi:10.1038/ng.2802.Meta-analysis
- Johansson FD, Shalit U, Sontag D. Learning Representations for Counterfactual Inference. NIPS. 2018. doi:10.1093/eurheartj/ehp595
- Wu J, Graff A, Deckman J, et al. Ultrafast Brain Segmentation using a 3D Fully Convolutional Neural Network for Risk Stratification of Cognitive Impairment and Dementia. ISMRM. Submitted 2019.
Figures