3297
Minimum Requirements for Diffusion Tensor Imaging (DTI) for a Longitudinal Trial1Imaging Institute, The Cleveland Clinic, Cleveland, OH, United States, 2Neurological Institute, The Cleveland Clinic, Cleveland, OH, United States
Synopsis
This study examines the optimal number of diffusion-weighting gradients for using DTI as an outcome in a multicenter clinical trial. The results suggest that 6 directions may be sufficient for large, simple fiber tracts. This finding may help simplify the implementation of DTI into clinical trials.
Introduction
The optimal number of gradient directions required for DTI has been the subject of much study. Sampling more than the minimum of 6 directions can reduce the variability of tissue microstructure parameters1. A re-examination of this issue found, for relatively simple tracts lacking crossing fibers, 6 directions can be enough2. In planning a longitudinal study, variability over time is an additional factor that must be considered. Here, we retrospectively examine a large dataset from a longitudinal DTI trial3,4 to understand the impact of the number of gradient directions.Methods
As part of the SPRINT-MS trial, 188 patients completed 5 scan sessions (0, 24, 48, 72 and 96 weeks). DTI was acquired at 3 tesla (64 diffusion-weighting gradient directions at b=700sec/mm2, 8 b=0, 2.5mm isotropic voxels) at 26 sites. At one site, only 55 directions were acquired, affecting data from one subject. Probabilistic tractography was performed to delineate pyramidal tracts, and DTI measures of microstructure (fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD) and axial diffusivity (AD)) were calculated within the tracts5. A subset of 12 directions and 1 b=0 image was then taken from each dataset, followed by tractography and estimates of tissue microstructure. Tractography and microstructure estimates were repeated using a subset of 6 directions and 1 b=0 image. For one subject at one timepoint, tractography failed when using the 12 direction dataset, so all data from this subject was excluded.Results
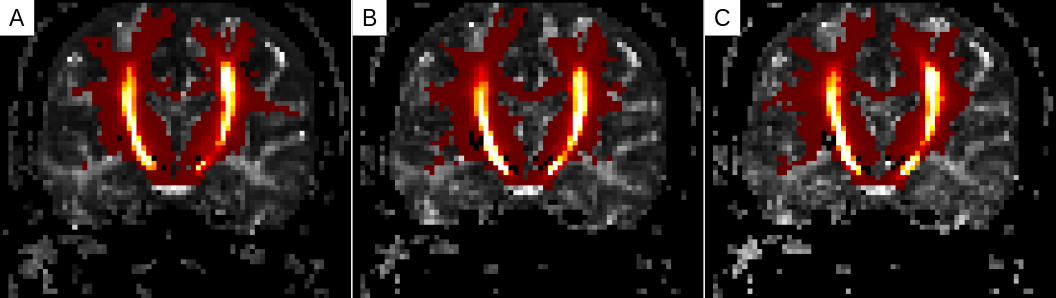
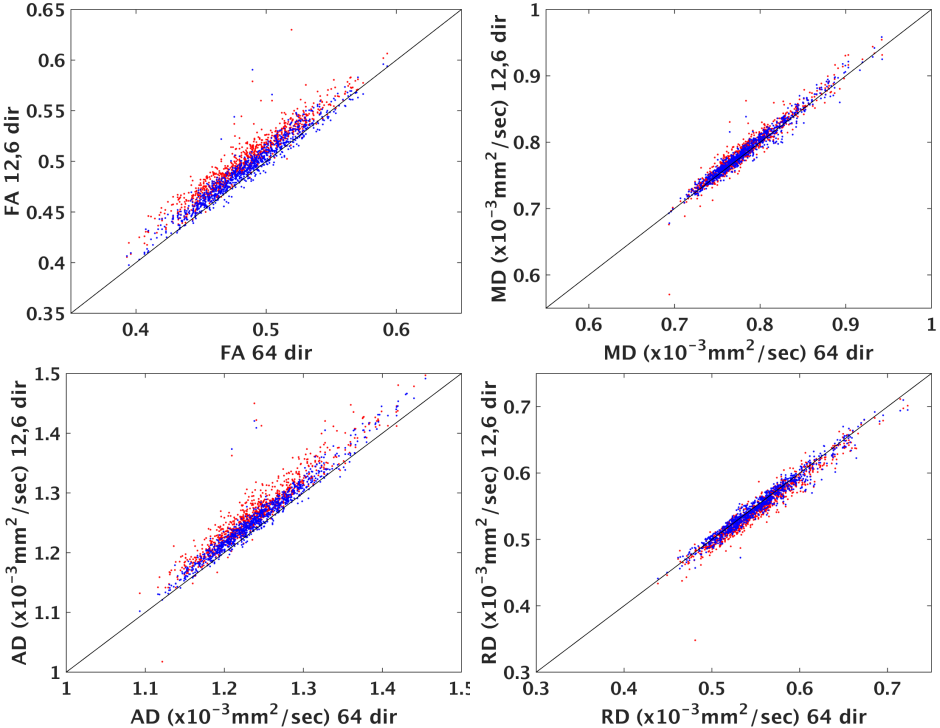
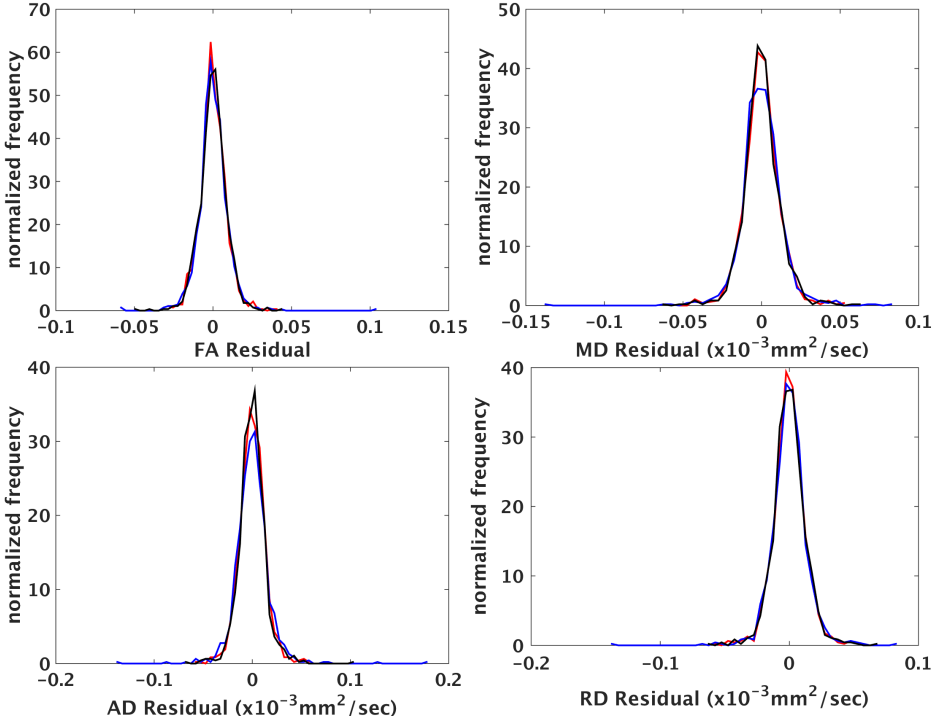
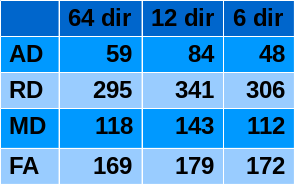
Figure 1 shows track density maps. The spatial arrangement of the fiber tracks is consistent. Figure 2 compares tissue microstructure parameters for all subjects and timepoints. Correlation is high (R2 > 0.90), but AD and FA are systematically higher with fewer directions. Figure 3 shows normalized histograms of residuals around regression lines and show no significant difference (paired t-test, p > 0.99) with number of directions. Figure 4 shows sample size estimates for a two-armed longitudinal trial assuming difference between groups of 1% in change per year over 12 months (α=0.05, power=0.8)6. Differences are largely driven by differences in correlation between timepoints, not baseline variance.Discussion and Conclusion
The results suggest that 6 directions perform as well as 64 directions when assessing the pyramidal tract for cross-sectional studies (figure 2) and for longitudinal studies (figure 3,4). This is surprising because more directions are expected to limit variability due to changes in orientation of anisotropic white matter with patient position over time while improving signal-to-noise-ratio. However, biological noise may dominate variability2. Orientational variation might be limited by the relatively low b-value. Use of only 6 directions precludes examination of white matter pathways that include fiber crossings. However, a minimal DTI acquisition has practical advantages. Short scan times reduce the risk of motion and cost. Special licenses associated with more directions can be avoided, increasing the number of eligible sites and enrollment. In conclusion, a minimal DTI acquisition may be appropriate for some clinical trials.Acknowledgements
We acknowledge support from the National Institute of Neurological Disorders and Stroke (U01NS082329), National Multiple Sclerosis Society (RG 4778-A-6) and from MediciNova through a contract with the National Institutes of Health.References
1. Jones, D. K. The effect of gradient sampling schemes on measures derived from diffusion tensor MRI: a Monte Carlo study. Magn Reson Med 2004; 51(4):807-815.
2. Lebel, C., Benner, T. & Beaulieu, C. Six is enough? Comparison of diffusion parameters measured using six or more diffusion-encoding gradient directions with deterministic tractography. Magn Reson Med 2012; 68(2):474-483.
3. Fox, R. J., Coffey, C. S., Conwit, R., Cudkowicz, M. E., Gleason, T., Goodman, A., Klawiter, E. C., Matsuda, K., McGovern, M., Naismith, R. T., Ashokkumar, A., Barnes, J., Ecklund, D., Klingner, E., Koepp, M., Long, J. D., Natarajan, S., Thornell, B., Yankey, J., Bermel, R. A., Debbins, J. P., Huang, X., Jagodnik, P., Lowe, M. J., Nakamura, K., Narayanan, S., Sakaie, K. E., Thoomukuntla, B., Zhou, X., Krieger, S., Alvarez, E., Apperson, M., Bashir, K., Cohen, B. A., Coyle, P. K., Delgado, S., Dewitt, L. D., Flores, A., Giesser, B. S., Goldman, M. D., Jubelt, B., Lava, N., Lynch, S. G., Moses, H., Ontaneda, D., Perumal, J. S., Racke, M., Repovic, P., Riley, C. S., Severson, C., Shinnar, S., Suski, V., Weinstock-Guttman, B., Yadav, V., Zabeti, A. & Investigators, N. S.-M. T. Phase 2 Trial of Ibudilast in Progressive Multiple Sclerosis. N Engl J Med 2018; 379(9):846-855.
4. Fox, R. J., Coffey, C. S., Cudkowicz, M. E., Gleason, T., Goodman, A., Klawiter, E. C., Matsuda, K., McGovern, M., Conwit, R., Naismith, R., Ashokkumar, A., Bermel, R., Ecklund, D., Koepp, M., Long, J., Natarajan, S., Ramachandran, S., Skaramagas, T., Thornell, B., Yankey, J., Agius, M., Bashir, K., Cohen, B., Coyle, P., Delgado, S., Dewitt, D., Flores, A., Giesser, B., Goldman, M., Jubelt, B., Lava, N., Lynch, S., Miravalle, A., Moses, H., Ontaneda, D., Perumal, J., Racke, M., Repovic, P., Riley, C., Severson, C., Shinnar, S., Suski, V., Weinstock-Gutman, B., Yadav, V. & Zabeti, A. Design, rationale, and baseline characteristics of the randomized double-blind phase II clinical trial of ibudilast in progressive multiple sclerosis. Contemp Clin Trials 2016; 50(166-177.
5. Lowe, M. J., Beall, E. B., Sakaie, K. E., Koenig, K. A., Stone, L., Marrie, R. A. & Phillips, M. D. Resting state sensorimotor functional connectivity in multiple sclerosis inversely correlates with transcallosal motor pathway transverse diffusivity. Hum Brain Mapp 2008; 29(7):818-827.
6. Harrison, D. M., Caffo, B. S., Shiee, N., Farrell, J. A., Bazin, P. L., Farrell, S. K., Ratchford, J. N., Calabresi, P. A. & Reich, D. S. Longitudinal changes in diffusion tensor-based quantitative MRI in multiple sclerosis. Neurology 2011; 76(2):179-186.
Figures