3284
Widespread Structural and Functional Brain Connectivity Changes and Behavioral Relevance in Glaucoma1Department of Ophthalmology, New York University School of Medicine, New York, NY, United States, 2Department of Kinesiology, East Carolina University, Greenville, NC, United States, 3Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA, United States, 4Department of Ophthalmology, University of Pittsburgh, Pittsburgh, PA, United States, 5Department of Radiology, New York University School of Medicine, New York, NY, United States
Synopsis
Glaucoma is the second leading cause of blindness worldwide, yet its effects on the brain structure and function and the related behavioral relevance remain unclear. This study shows that glaucoma patients present reduced structural integrity in white matter around the supramarginal gyrus, as well as reduced functional connectivity between supramarginal gyrus and visual occipital and superior sensorimotor areas when compared to healthy controls. Furthermore, decreased functional connectivity between supramarginal gyrus and
Introduction
Glaucoma is the world’s second leading cause of blindness and is projected to affect 111.8 million people worldwide by 2040.1 Glaucoma typically presents elevated intraocular pressure, progressive retinal ganglion cell death, and irreversible vision loss, making the eye the main focus for therapies and research. Recent neuroimaging research suggests the occurrence of changes in a number of brain structures in glaucoma,2 yet the behavioral relevance remains unclear. Glaucoma patients also present an increased risk of falls,3,4 which has been traditionally thought to be attributed to the underlying visual impairments. However, another mechanism may be central in origin. Specifically, the multisensory processing of inputs from the visual, vestibular and somatosensory systems may be impaired.5,6 In this study, we assess the structural and functional brain connectivity in glaucoma in combination with dynamic posturography to examine associations between brain changes and postural control.Methods
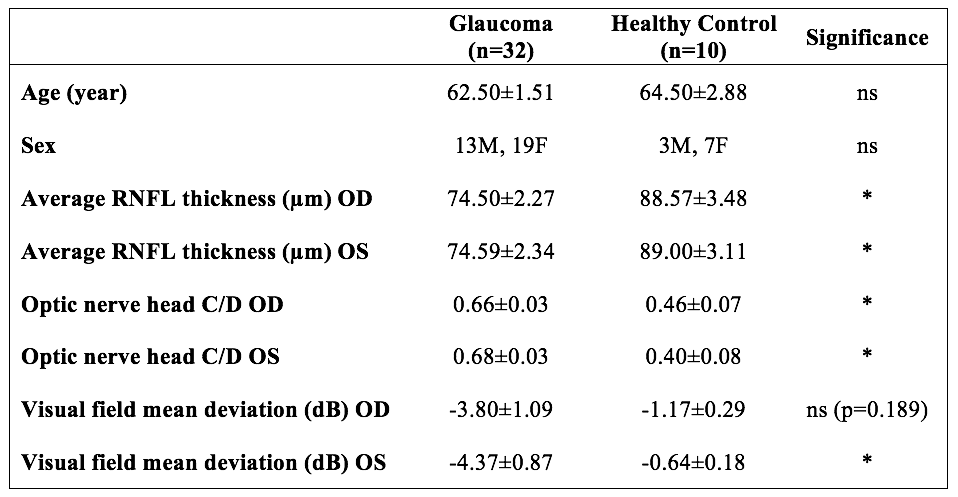
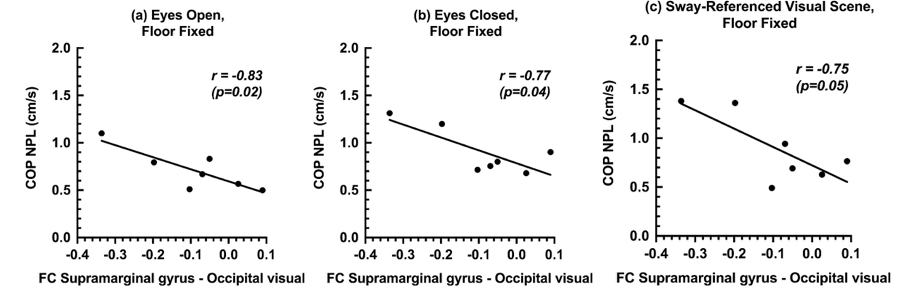
Early glaucoma subjects (n=32) and healthy controls (n=10) underwent clinical ophthalmic assessments including spectral-domain optical coherence tomography (OCT) and standard automated perimetry (SAP), followed by Siemens 3-Tesla anatomical MRI (MPRAGE, resolution=1x1x1mm3), diffusion tensor MRI [DTI; b=850 s/mm2 and one b = 0 s/mm2 (b0); 12 diffusion directions] and task-free functional connectivity MRI (tf-fMRI; 8 min) with eyes closed at rest. From clinical OCT reports, average peripapillary retinal nerve fiber layer (RNFL) thickness and optic nerve head cup-to-disc ratio (C/D) were extracted from both left (OS) and right (OD) eyes, while visual field mean deviation (VF-MD) values were extracted from SAP reports. For tf-fMRI, the Functional Connectivity (CONN) toolbox was used for data preprocessing and region-of-interest (ROI) analyses. Brain ROIs were specified by the Automated Anatomical Labeling (AAL) and the Harvard-Oxford Atlas. Seed-based analysis was performed by calculating the temporal correlation between the defined set of seed voxels and other voxels. Age was selected as a covariate to control for group differences. For DTI, preprocessing was performed with Freesurfer’s dt_recon function followed by non-linear registration of the fractional anisotropy (FA) maps into the MNI152 standard space for voxelwise comparisons using tract-based spatial statistics (TBSS). Additionally, a subset of 7 glaucoma subjects underwent dynamic posturography to assess postural stability, specifically the multisensory integration abilities relevant for balance. An adapted Sensory Organization Test (SOT) was used on the Equitest posture platform (Neurocom, Inc).7-9 This platform is capable of rotating the floor under the subject and/or altering the subjects’ visual scene in direct proportion to the individual’s sway, a sensory perturbation referred to as sway-referencing, thereby reducing the reliability of somatosensory information from the ankle and/or from vision, respectively. From this test, the average sway velocity in the anterior-posterior direction was assessed using time-normalized path length (NPL) of the center of pressure (COP).Results
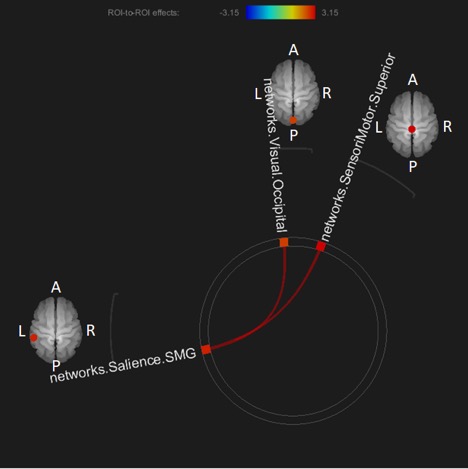
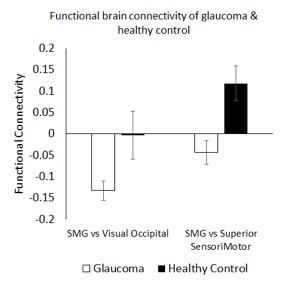
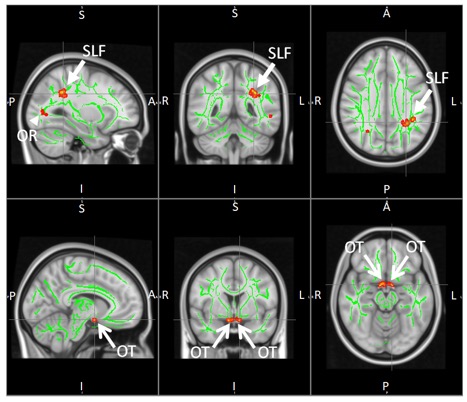
There were significant differences in clinical ophthalmic assessments between glaucoma patients and healthy controls while no apparent age or gender difference was observed (Figure 1). In tf-fMRI, the left supramarginal gyrus (SMG) had lower functional connectivity with the visual occipital area (VO) and superior sensorimotor area (SSM) in glaucoma patients than healthy controls (Figures 2-3). Furthermore, negative associations were found between sway velocity during posturography and functional connectivity between SMG and VO in glaucoma patients (Figure 4). In DTI, lower FA was observed in the optic tracts and optic radiations of the primary visual pathway, as well as the superior longitudinal fasciculus (SLF) around the left SMG in glaucoma patients compared to healthy controls (Figure 5).Discussion
The SMG is an important brain region for the maintenance of balance and gait control10,11 and is structurally connected to the SLF.12 The decreased functional connectivity between SMG and the visual and sensorimotor regions observed in glaucoma subjects suggests that functional brain reorganization is taking place in these areas, and consequently could be responsible in part for the increased fall risk in glaucoma. This hypothesis is bolstered by the lower FA observed in the SLF around the SMG of glaucoma subjects. Furthermore, the significant brain-behavior associations in glaucoma subjects suggest that decreased functional connectivity between SMG and VO could be a factor in the ability to control balance, especially when visual and somatosensory information becomes unavailable or impaired.Conclusion
The neurobehavioral findings suggest the involvement of brain areas responsible for vision and balance in early stages of glaucoma. Decreased structural and functional connectivity in SMG, VO and SSM may negatively impact postural control in glaucoma patients. Altered brain coordination may be a potential mechanism behind increased risk of falls in glaucoma.Acknowledgements
This work was supported in part by the National Institutes of Health R01-EY028125 (Bethesda, Maryland); BrightFocus Foundation G2013077 and G2016030 (Clarksburg, Maryland); and Research to Prevent Blindness/Stavros Niarchos Foundation International Research Collaborators Award (New York, New York)References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 2014;121(11):2081-2090.
2. Murphy MC, Conner IP, Teng CY, et al. Retinal Structures and Visual Cortex Activity are Impaired Prior to Clinical Vision Loss in Glaucoma. Sci Rep 2016;6:31464.
3. Lamoureux EL, Chong E, Wang JJ, et al. Visual impairment, causes of vision loss, and falls: the singapore malay eye study. Invest Ophthalmol Vis Sci 2008;49(2):528-533.
4. Patino CM, McKean-Cowdin R, Azen SP, et al. Central and peripheral visual impairment and the risk of falls and falls with injury. Ophthalmology 2010;117(2):199-206 e191.
5. Maurer C, Mergner T, Peterka RJ. Multisensory control of human upright stance. Exp Brain Res 2006;171(2):231-250.
6. Black AA, Wood JM, Lovie-Kitchin JE, Newman BM. Visual impairment and postural sway among older adults with glaucoma. Optom Vis Sci 2008;85(6):489-497.
7. Redfern MS, Jennings JR, Martin C, Furman JM. Attention influences sensory integration for postural control in older adults. Gait Posture 2001;14(3):211-216.
8. O'Connell C, Mahboobin A, Drexler S, et al. Effects of acute peripheral/central visual field loss on standing balance. Exp Brain Res 2017;235(11):3261-3270.
9. Cham R, Perera S, Studenski SA, Bohnen NI. Striatal dopamine denervation and sensory integration for balance in middle-aged and older adults. Gait Posture 2007;26(4):516-525.
10. Karim H, Fuhrman SI, Sparto P, Furman J, Huppert T. Functional brain imaging of multi-sensory vestibular processing during computerized dynamic posturography using near-infrared spectroscopy. Neuroimage 2013;74:318-325.
11. Ben-Shabat E, Matyas TA, Pell GS, Brodtmann A, Carey LM. The Right Supramarginal Gyrus Is Important for Proprioception in Healthy and Stroke-Affected Participants: A Functional MRI Study. Front Neurol 2015;6:248.
12. Wang X, Pathak S, Stefaneanu L, Yeh FC, Li S, Fernandez-Miranda JC. Subcomponents and connectivity of the superior longitudinal fasciculus in the human brain. Brain Struct Funct 2016;221(4):2075-2092.
Figures