3264
Method for vessel selection effects the outcome and reproducibility of velocity and pulsatility measures in cerebral penetrating arteries1Radiology, UMC Utrecht, Utrecht, Netherlands, 2Spinoza Centre for Neuroimaging, Amsterdam, Netherlands, 3Neurology, UMC Utrecht, Utrecht, Netherlands
Synopsis
Measuring the function of the cerebral small vessels can greatly benefit our understanding of cerebral small vessel disease. Recent research enabled the assessment of blood flow velocity and pulsatility in the perforating arteries of the cerebral white matter in healthy subjects. However, in patients this method requires manual elimination of artifacts. This paper explores various methods for excluding false positives. The reproducibility of the velocity, pulsatility and number of selected vessels was investigated in a test-retest study. Results show that the reproducibility of these outcome measures highly depends on the chosen method for vessel selection.
Introduction
Cerebral small vessel disease is a widespread neurological disorder in which the small vessels and the cerebral circulation in the brain are affected [1]. Therefore, measuring the function of these vessels can make a substantial contribution to our understanding of the physiology of the cerebral microcirculation. Previously, a method was developed to detect small perforating arteries in the cerebral white matter (WM), which yields measurements of the blood flow velocity (Vmean) and pulsatility index (PI) [2,3]. However, although this method offers automated analysis in healthy controls, application in elderly patients often shows reduced quality, which requires manual adjustments of the ROIs to exclude artifacts (mainly ghosts from large arteries)(Figure 1)[4]. In this exploratory study, three methods for vessel selection were investigated and the reproducibility of these methods was assessed regarding the outcome measures Vmean, PI and the number of selected perforators (Nselected).Methods
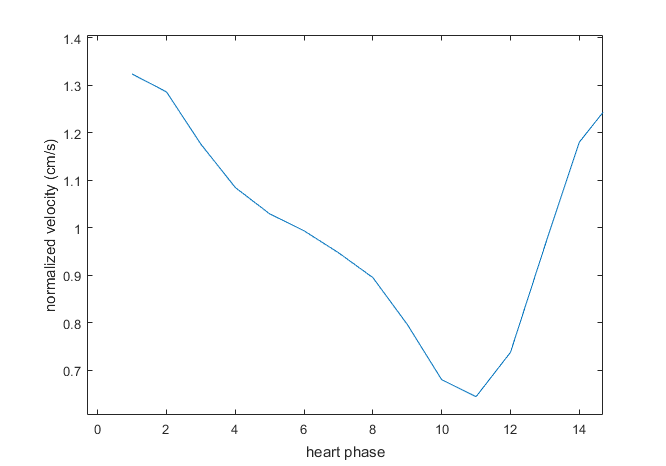
15 patients with either vascular cognitive impairment or carotid occlusive disease (69 ± 9, 10 male) and 10 healthy controls (68 ± 8, 5 male) were included. Written informed consent was obtained from all patients and controls. All subjects were scanned with a 7T MRI (Philips) with a 32-channel receive head coil (Nova Medical) with the previously described retrospectively gated 2D Qflow sequence (Venc cm/s, 0.3mm in plane resolution, see Geurts et al [3] for details). To obtain reproducibility measures, the scan was repeated (without repositioning). Processing steps were as described before [3]. The method of Geurts et al [3] was used as the initial uncensored vessel selection, in which vessels are automatically selected within a segmented white matter mask (SPM12) based on their mean velocity-to-noise ratio. We used a 50% probability threshold for WM segmentation. Subsequently, two additional censoring methods were explored: automated censoring, removing only small vessels detected in the ‘ghosting path’ (in the phase encoding direction) of large arteries, and a manual censoring method, including only vessels which were subjectively judged to show a representative velocity curve (Figure 2). The automatic censoring method is illustrated in Figure 3. In short: inhomogeneity correction was applied to the mean (over the cardiac cycle) magnitude image by applying a median filter (window: 70x70) and subtracting the median filtered magnitude from the original mean magnitude. Large blood vessels were automatically identified by applying an intensity threshold and selecting only clusters of more than two pixels. Subsequently, these clusters were dilated and extended in the phase encoding direction to create vertical stripes that were removed from the WM mask. Reproducibility was assessed by computing the coefficient of repeatability (CoR) with Bland-Altman analysis.Results and discussion
The method of vessel selection had a considerable effect on the outcome measures and their reproducibility between scans, as can be seen in Table 1. For patients, automated censoring and manual censoring included 54% and 12% of the vessels included in the uncensored selection, respectively. For controls, this was 52.2% and 19%. As the number of selected vessels declines, the absolute reproducibility of Vmean and of PI decreases (higher CoR). This may indicate that the noise, present in the signal of each individual vessel, averages out for a larger number of included vessels. However, for the PI, the relative reproducibility increases (lower %CoR) with lower Nselected. This may reflect (especially for the manual censoring) that the selected vessels have more similarly aligned minima and maxima (Figure 2), which avoids cancelation of pulsations due to noise. The outcomes for PI for the uncensored vessel selection given in Table 1 are lower compared to the values calculated in by Geurts et al [3]. This difference is probably due to a higher probability threshold for the WM mask (Geurts et al [3] used a 95% probability threshold, yielding more conservative ROIs). The current ROIs contained more peripheral WM areas in small gyri, which are more prone to noise from large vessels in the CSF and show lower SNR due to relative lower flip angles at 7T. Thus, more noisier vessels may be included, contributing to the lower observed PIs in the current analysis.Conclusion
These results show that Nselected and PI greatly depend on the method used for vessel selection, while Vmean appears to be more insensitive. Vessel selection for velocity and pulsatility measurement in patients remains challenging, and special attention should be paid to the method for vessel selection. Future research will focus on improved algorithms for distinguishing true vascular signals from artifacts and noise, and robust selection of regions of interest even in the case of subject motion between the acquisition of the T1 scan and the 2D Qflow measurements.Acknowledgements
This work was supported by the European Research Council, ERC grant agreement nᵒ337333 (JZ) and by the Horizon 2020 program of the European Union, grant agreement n° 666881.References
[1] Pantoni L. Cerebral small vessel disease: from pathogenesis and clini- cal characteristics to therapeutic challenges. Lancet Neurol 2010;9: 689–701.10.
[2] Bouvy WH, Geurts LJ, Kuijf HJ, Luijten PR, Kapelle LJ, Biessels GJ, Zwanenburg JJM. Assessment of blood flow velocity and pulsatility in cerebral perforating arteries with 7-T quantitative flow MRI. NMR Biomed 2016:29:1295-1304.
[3] Geurts LJ, Biessels GJ, Luijten PR, Zwanenburg JJM. Better and faster velocity pulsatility assessment in cerebral white matter perforating arteries with 7T quantitative flow MRI through improved slice profile, aquisition scheme and postprocessing. Magn. Reson. Med. doi:10.1002/mrm.26821.
[4] Geurts LJ, Biessels GJ, Luijten PR, Klijn CJ, Zwanenburg JJM. Increased pulsatility in cerebral perforating arteries in patients with lacunar infarction or deep intracerebral hemorrhage, an explorative 7T MRI study. In: Annual Meeting of the International Society of Magnetic Resonance; 2018; Paris: International Society of Magnetic Resonance; 2018. p. 1146.
Figures