3261
Evaluation of collateral circulation in intracranial atherosclerosis using random vessel-encoded arterial spin labeling1USC Stevens Neuroimaging and Informatics Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 2Department of Radiology, Zhengzhou University People’s Hospital & Henan Provincial People’s Hospital, Zhengzhou, China, 3Henan Key Laboratory for Medical Imaging of Neurological Diseases, Zhengzhou, China
Synopsis
Collateral circulation plays an important role in predicting the clinical outcomes and risk of recurrent stroke in patients with stroke and transient ischemic attack (TIA). In this study, we evaluated the clinical utility of random vessel-encoded ASL (
Purpose
Collateral circulation1 plays an important role in predicting the clinical outcomes in patients with stroke and transient ischemic attack (TIA). Digital subtraction angiography (DSA) remains the gold standard to evaluate collaterals in spite of its invasive nature. Recently, arterial spin labeled (ASL) MRI has become a potential alternative to assess the collateral circulation2,3. Especially, vessel-encoded ASL4 (VE-ASL) has the capability of detecting the perfusion territories from individual feeding arteries. However, prior knowledge of the spatial coordinates of feeding arteries is always required in VE-ASL which may hamper its clinical utilities. To overcome the limitation, random VE-ASL5,6 (rVE-ASL) has been developed, which can detect the feeding arteries as well as corresponding vascular territories without prior spatial information. In this study, we aim to evaluate the clinical value of rVE-ASL for the assessment of vascular territory especially collateral circulation in patients with stroke and TIA through comparison with DSA.Methods
Patients
The criteria of patient enrollment included individuals who had clinical evidence of ischemic stroke or transient ischemic attack within 30 days. Angiographic evidence (e.g. DSA, CTA or TOF-MRA) showed at least one vascular stenosis as verified by neuroradiologists. The patients who didn’t receive any angiography or had severe head motion during MRI scan were excluded.
Experiment
All the scans were performed on a Siemens Prisma 3T scanner. The clinical routine scans included T1, T2, FLAIR, DWI, and TOF. Random VE-ASL with background suppressed (BS) single-shot 3D GRASE acquisition was collected on each patient with the following parameters: FOV= 256×256 mm2, matrix size=96×96, TE/TR=36/3660ms, labeling duration=1.5s, post-labeling delay=1.5s, 12 slices with slice thickness of 8 mm, 60 pairs of encoding steps with random orientation, phase and wavelength and two additional pairs of global label/control, leading to a total scan time of 7min 30s.
Image analysis
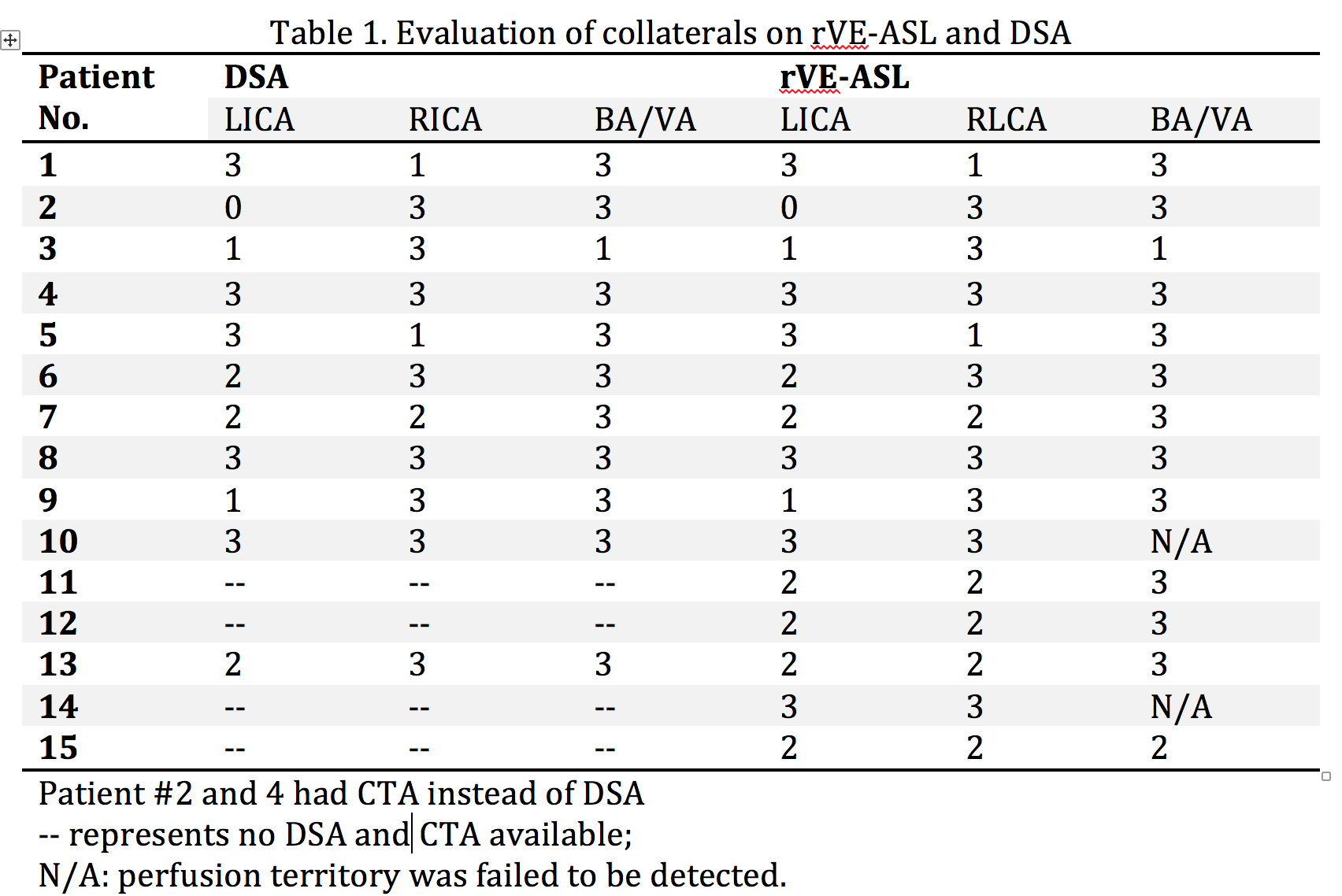
The locations of feeding arteries were identified by the correlation coefficient (CC) between the acquired perfusion signal and a database of predicted signal distributions5. The corresponding perfusion territorial maps were subsequently generated based on the highest CC in each voxel. Collaterals were evaluated in the left intracranial carotid artery (LICA), right intracranial carotid artery (RICA), and basilar artery (BA) territories on rVE-ASL and DSA images independently according to the following criteria2: 0: poor, no collateral circulation; 1: intermediate, partial collateral flow to the ischemic region; 2: good, full collateral flow to the site of occlusion; 3: normal antegrade flow.
Results and Discussion
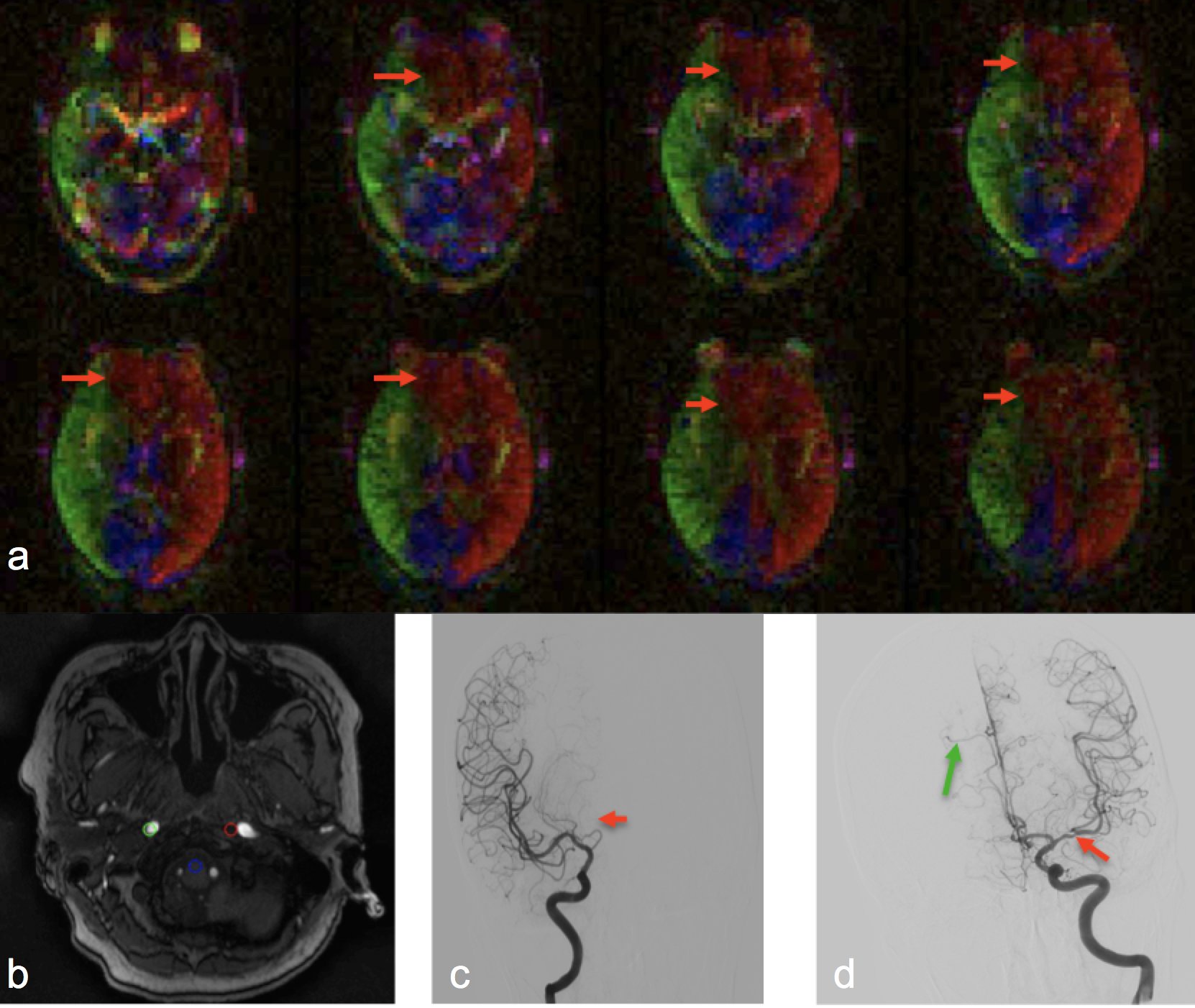
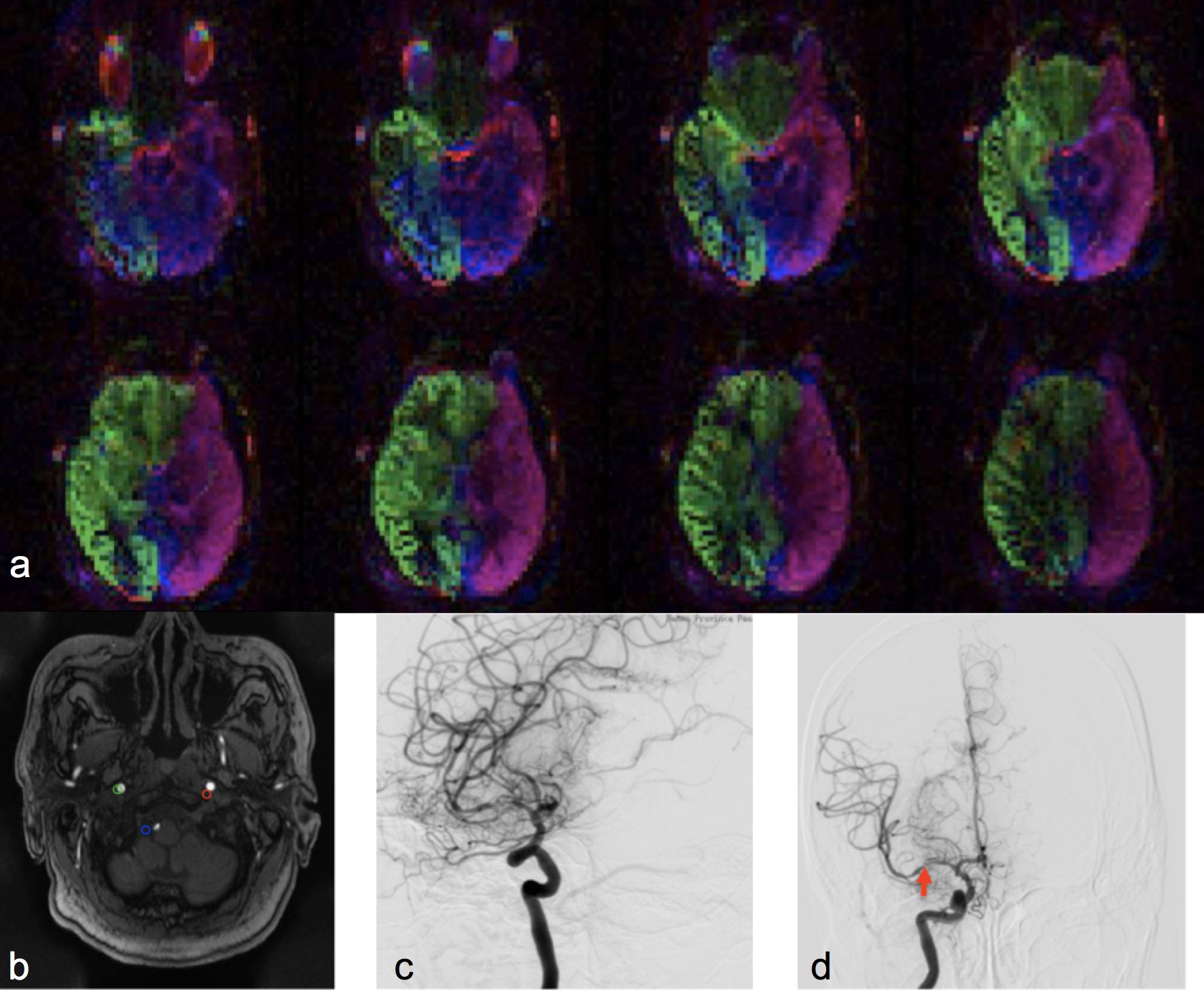
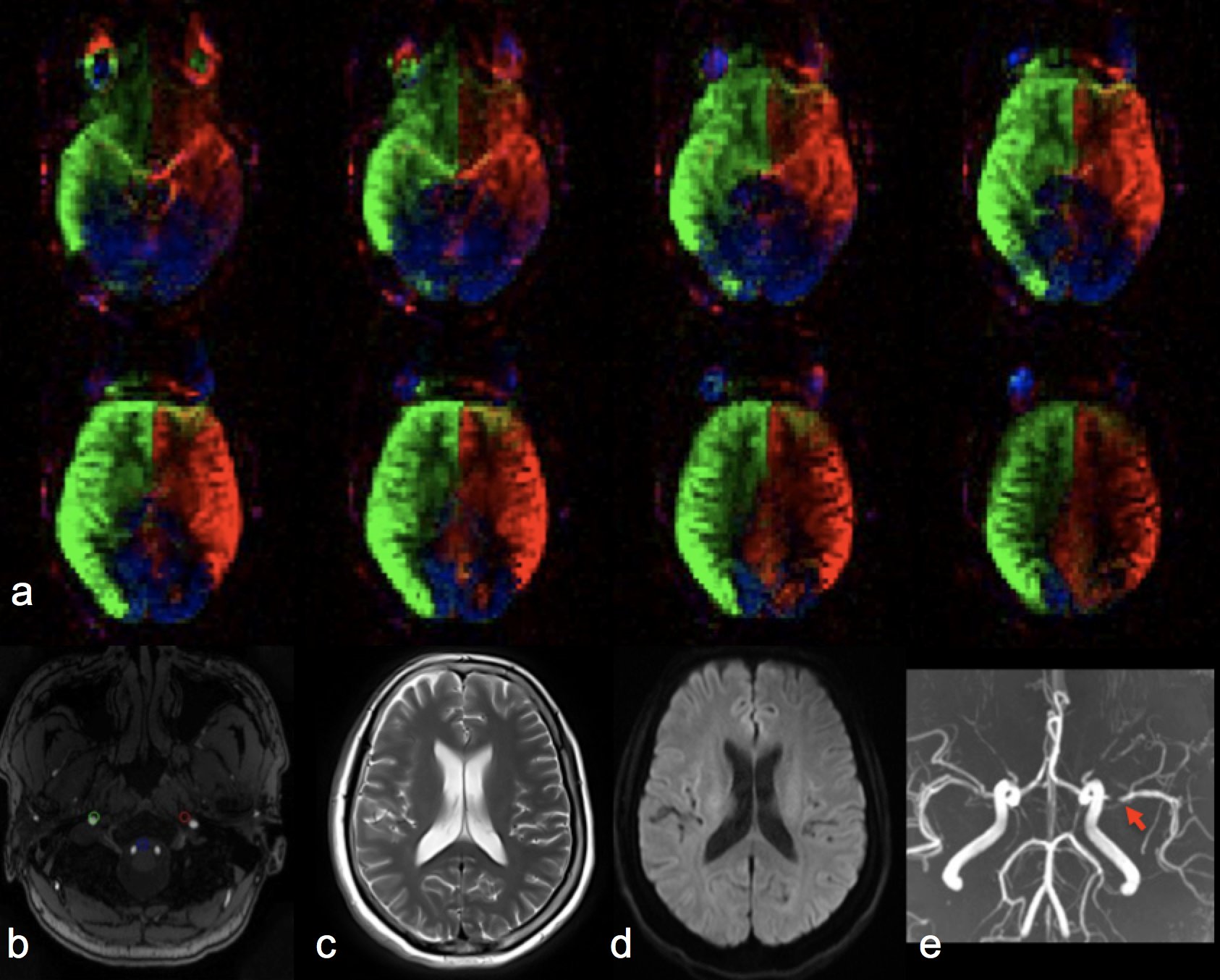
15 patients were enrolled in this study including 4 strokes and 11 TIAs. All the patients had moderate to severe intracranial stenosis (n=12) or occlusion (n=3). Figure 1 displays the perfusion territorial map (Fig 1a), locations of feeding arteries (Fig 1b) and DSA (Fig1 c-d) from one patient who had an occlusion in A1 segment of the right anterior cerebral artery (RACA) and mild stenosis in M1 segment of the left middle cerebral artery (LMCA). Collaterals for the occluded RACA were formed through left ACA. No collaterals were detected due to the mild stenosis in LMCA. Figure 2 shows a patient with severe stenosis in M1 segment of the right middle cerebral artery (RMCA). No obvious collaterals were detected in this case. However, asymmetric perfusion territories were noticed between left and right ICA, which was confirmed by DSA. Figure 3 shows another case who had TIA a month ago before MRI scan. A severe stenosis in M1 of LMCA was visualized on TOF images. However, rVE-ASL shows normal perfusion territories.
The scores of collaterals by rVE-ASL and DSA were listed in Table 1, which are in good agreement with each other. As noted in the Table1, the perfusion territories fed by ICA were successfully obtained from all the patients and were quite consistent with DSA findings. However, the vertebral arteries (VA) and associated perfusion territories were failed to be detected in two cases, which was probably caused by reduced labeling efficiency due to the geometry features of VA (not perpendicular to the labeling plane) and reduced flow due to the presence of stenosis in VA.
Conclusion
Random VE-ASL could be a valuable tool to assess the collateral circulation in patients with stroke and TIA. It offers several advantages over conventional VE-ASL including no requirement of prior spatial knowledge of feeding arteries and improved robustness to off-resonance. The collateral evaluation using rVE-ASL was in good accordance with that of DSA, especially in the detection of perfusion territories of ICA. Further optimization is needed to improve the robustness of VA/BA detection.Acknowledgements
This work is supported by grants of AHA16SDG29630013, NIH K25AG056594, NNSFC (81720108021, 81772009,81601466,81641168, 31470047), National Key R&D Program of China (YS2017YFGH000397), Scientific and Technological Research Project of Henan Province (182102310162) and the Key Project of Henan Medical Science and Technology Project (201501011).References
[1]. Liebeskind DS, Collateral circulation. Stroke. 2003 Sep;34(9):2279-84.
[2]. Chng SM, Petersen ET, Zimine I, Sitoh YY, Lim CC, Golay X. Territorial arterial spin labeling in the assessment of collateral circulation: comparison with digital subtraction angiography. Stroke. 2008 Dec;39(12):3248-54.
[3]. Lyu J, Ma N, Liebeskind DS, Wang DJ, Ma L, Xu Y, Wang T, Miao Z, Lou X. Arterial Spin Labeling Magnetic Resonance Imaging Estimation of Antegrade and Collateral Flow in Unilateral Middle Cerebral Artery Stenosis. Stroke. 2016 Feb;47(2):428-33.
[4]. Wong EC. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magn Reson Med. 2007 Dec;58(6):1086-91.
[5]. Wong EC, Guo J. Blind detection of vascular sources and territories using random vessel encoded arterial spin labeling. MAGMA. 2012 Apr;25(2):95-101.
[6]. Yan L, Yu S, Guo J, Liebeskind DS, Saver JL, Salamon N, Yao N, Sheth S, Liang C, Wong EC, and Wang DJ. Evaluation of random vessel-encoded ASL in both healthy subjects and stroke patients. ISMRM2014, p3849.
Figures