3259
Is It Necessary for Patients with Internal Carotid Artery Occlusion to Undergo 3D Head-neck Combined Vessel Wall Cardiovascular Magnetic Resonance Imaging?Jin Zhang1, Huilin Zhao1, Beibei Sun1, Xiaosheng Liu1, Xiaoyue Zhou2, Xihai Zhao3, Chun Yuan4, and Jianrong Xu1
1Renji Hospital Affiliated to Shanghai Jiaotong University, Shanghai, China, 2MR Collaboration, Siemens Healthcare Ltd., Shanghai, China, 3Biomedical Engineering & Center for Biomedical Imaging Research, Tsinghua University, Beijing, China, 4Radiology, University of Washington, Seattle, WA, United States
Synopsis
Definite diagnosis of internal carotid artery occlusion no longer satisfies neurosurgeons’ treatment needs for vascular recanalization. This study sought to investigate what information provided by 3D head-neck combined vessel wall cardiovascular magnetic resonance imaging could be useful for neurosurgeon to make the therapy plan. Our study turned out that 3D MR vessel wall imaging is capable of diagnosing internal carotid artery occlusion, and patients with short extent of occlusion are benefit from the vascular recanalization therapy. Our results suggest it is useful for those patients to undergo 3D MR vessel wall imaging for making their therapy plan.
Introduction
Although digital subtraction angiography (DSA) remains the gold standard for diagnosing carotid occlusion, it appears powerless when asked for more messages of the affected vessels[1]. 3D head-neck combined vessel wall cardiovascular magnetic resonance imaging (CMRI) has developed to provide more information other than occlusion, such as the occlusion site, the distal vascular structure and the condition of ipsilateral middle cerebral artery[2]. In this study, we aimed to analyze the accuracy of 3D vessel wall CMRI compared with DSA and to figure out whether the information provided by 3D vessel wall CMRI is useful for the personalized treatment plan.Methods
Study Sample: A total of 22 patients who were diagnosed with internal carotid artery occlusion by conventional CT angiography, underwent DSA and MRI for further evaluation were recruited in the study. 18 patients proved to be internal carotid artery occlusion by both DSA and MRI were divided into interventional therapy group(n=8) and the conservative therapy group(n=10). MR Imaging: 3D head-neck combined vessel wall imaging was performed on a 3T whole-body MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) with a 20-channel head-neck coil and an 8-channel dedicated surface neck coil (Chenguang, Shanghai, China). A 3D variable-flip-angle TSE (SPACE) sequence and Angio 3D were used. Parameters of the relevant sequences were as follows: (1) SPACE[3,4]: TR/TE 800/11ms, Field of View (FOV) 260×208 mm2, slice thickness 0.70 mm, matrix 296×370, scan time 11 minutes and 13 seconds; (2) Angio 3D: TR/TE 3.27/1.20 ms, flip angle 25°, FOV 320×260 mm2, slice thickness 1.10 mm, matrix 256×384, scan time 16 seconds. When scanning this sequence, 0.1 mmol/kg of a gadolinium-based contrast agent (Magnevist, Bayer Healthcare, Berlin, Germany) was injected at a rate of 1.5 mL/s by power injector. DSA: An experienced neurointerventional physician carried out the DSA on the patients within one week of CMRI for confirmed diagnosis. Data Analysis: All head-neck combined vessel wall images were reviewed by an experienced neurovascular radiologist. The internal carotid artery was divided into seven segments, i.e., C1, cervical; C2, petrous; C3, lacerum; C4, cavernous; C5, clinoidal; C6, ophthalmic; and C7, communicating. The information of the occlusion site, the distal vascular collapse status and the ipsilateral middle cerebral artery was recorded.Results
A total of 22 patients (20 men, mean age 62.3 years old, range from 46 to 71 years) were included in this study. After analyzing the good consistency between the CMRI and the DSA examinations (Table 1), we selected 18 patients (17 men, mean age 61.7 years old, range from 46 to 71 years) which were diagnosed occlusion by both of the examinations for another round of statistical analysis (Table 2). There was no significant difference between the interventional therapy group and the conservative therapy group in lesion side, occlusion starting from C1, distal vascular collapse and ipsilateral MCA lesion (50% vs 60%, P=0.671; 62.5% vs 60.0%, P=0.914; 37.5% vs 10.0%, P=0.163; 12.5% vs 40.0%, P=0.196). Compared with the conservative therapy group, the interventional therapy group exhibited less prevalence of occlusion site over consecutive 3 segments (from starting segment to ending segment of occlusion) (12.5% vs 80.0%, P=0.004).Discussions
Our study showed that patients with occlusion site more than 3 segments, which indicating more risks or difficult for recanalization, had a higher rate of conservative therapy plan. 3D head-neck combined vessel wall CMRI can provide accurate occlusion site compared with DSA. We found that the presence of ipsilateral MCA lesion plays an unnegligible role for neurosurgeons to make the therapy plan. Neurosurgeons are more inclined to choose conservative treatment considering the efficacy under this circumstance. Larger smaple size and prospective study should be conducted for more reliable results in this issue.Conclusion
It will be benefit for patients with internal carotid artery occlusion to undergo 3D head-neck combined vessel wall CMRI, and the patients who turned out long extent of occlusion or ipsilateral MCA lesion may survive from these invasive angio examinations.Acknowledgements
Thank Cong Lin and Chuanzheng Li for their contribution of scanning patients and constructive advice.References
[1]. Han Y, Guan M, Zhu Z, et al. Assessment of longitudinal distribution of subclinical atherosclerosis in femoral arteries by three-dimensional cardiovascular magnetic resonance vessel wall imaging. J Cardiovasc Magn Reson. 2018;20(1):60. Published 2018 Sep 3. doi:10.1186/s12968-018-0482-7 [2]. Zhang N, Zhang F, Deng Z, et al. 3D whole-brain vessel wall cardiovascular magnetic resonance imaging: a study on the reliability in the quantification of intracranial vessel dimensions. J Cardiovasc Magn Reson. 2018;20(1):39. Published 2018 Jun 14. doi:10.1186/s12968-018-0453-z [3]. Xie G, Zhang N, Xie Y, et al. DANTE-prepared three-dimensional FLASH: A fast isotropic-resolution MR approach to morphological evaluation of the peripheral arterial wall at 3 Tesla. J Magn Reson Imaging. 2015;43(2):343-51. [4]. Xie Y, Yang Q, Xie G, Pang J, Fan Z, Li D. Improved black-blood imaging using DANTE-SPACE for simultaneous carotid and intracranial vessel wall evaluation. Magn Reson Med. 2015;75(6):2286-94.Figures
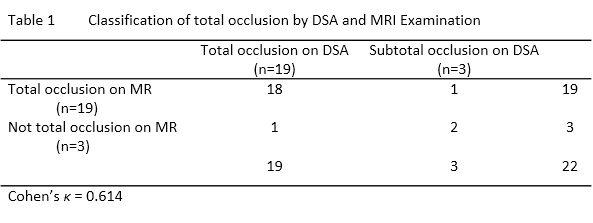
Classification of total occlusion by DSA and MRI
Examination
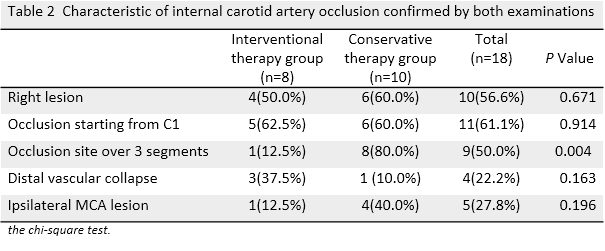
Characteristic
of internal carotid artery occlusion confirmed by both examinations
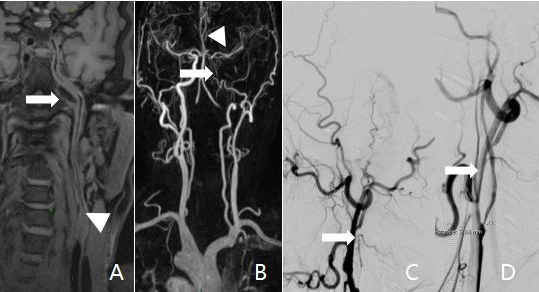
Example case of
interventional therapy of a 61-year-old man feeling intermittent dizziness with
slow response one month, which was also successfully recanalized. 3D MR vessel wall imaging showed more information of
occlusion site limited to C1 (triangle, A: curved from SPACE) with tenuous
lumen of distal vascular (arrow, A) and normal ipsilateral
MCA (triangle, B: MIP) than DSA (arrow, C: before recanalization and D:
after recanalazation).
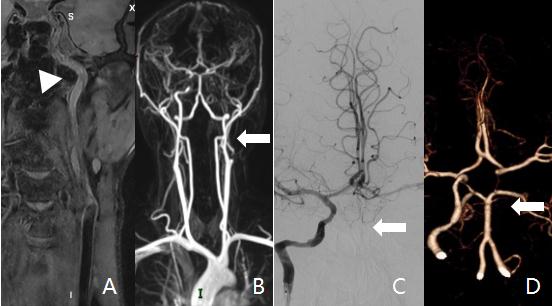
Example case of conservative therapy of a 46-year-old man
presented with right limb weakness and slurred speech one month. 3D
MR vessel wall imaging showed long occlusion from C1 to C6(triangle, A: curved
from SPACE) and normal ipsilateral MCA. B: MIP; C: DSA; D: CTA.