3255
Consistency of FLAIR vascular hyperintensity (FVH) and arterial transit artifact (ATA) in 3D ASL imaging in patients with unilateral MCA stenosis1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2GE Healthcare China, Beijing, China
Synopsis
Arterial spin labeling (ASL), a noncontrast method
of measuring CBF has become feasible in the clinical setting. Serpiginous
high intensity structures (ASL) are seen in the ischemic tissue on ASL, prior studies suggested that ATA may represent collateral flow. On the
other hand, FVHs are related to hemodynamic impairment and represent slow
retrograde flow in leptomeningeal collaterals. Our aim was to compare the consistency
of the occurrence of ATA relative to that of FVH in patients with proximal MCA
occlusion.
Target audience
Researchers interested in collateral circulation in patients with cerebral ischemia.Objective
To investigate correlation between FLAIR vascular hyperintensity (FVH) and arterial transit artifact (ATA) by using 3D ASL imaging in patients with the M1 segment of the middle cerebral artery (MCA) after severe stenosis or occlusion.Materials and Methods
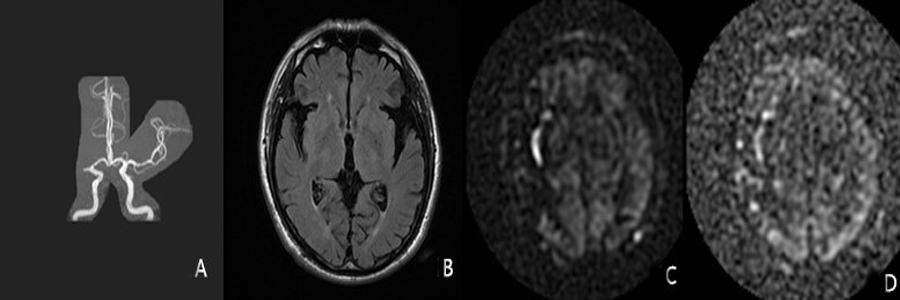
Forty-two patients with proximal (M1) middle cerebral artery severe stenosis or occlusion diagnosed by MRA or CTA were enrolled in this study, including 28 males and 14 females with a mean age of 63±14 years old. All performed MR protocols included conventional MRI, diffusion weighted imaging and 3D ASL imaging. Two radiologists counted the occurrence frequency of FVH on T2 FLAIR and ATA on the CBF image in PLD = 1.5 and PLD = 2.5, respectively. Correlation of FVH with ATA incidence and location were analyzed by Crosstabs and Chi square test. p≤0.05 means statistically significant.Results
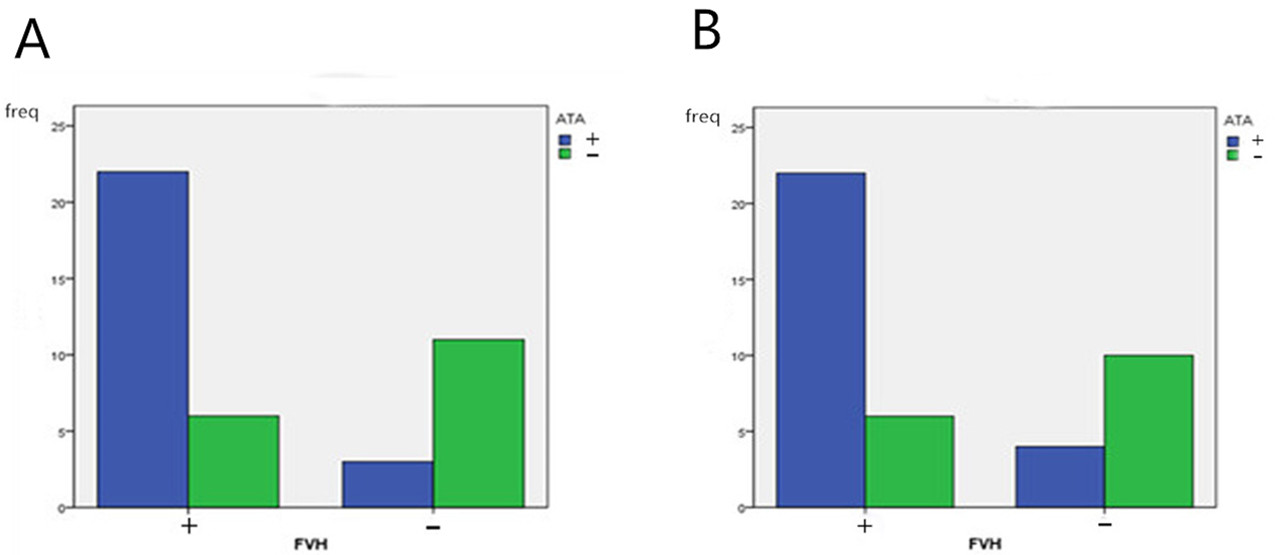
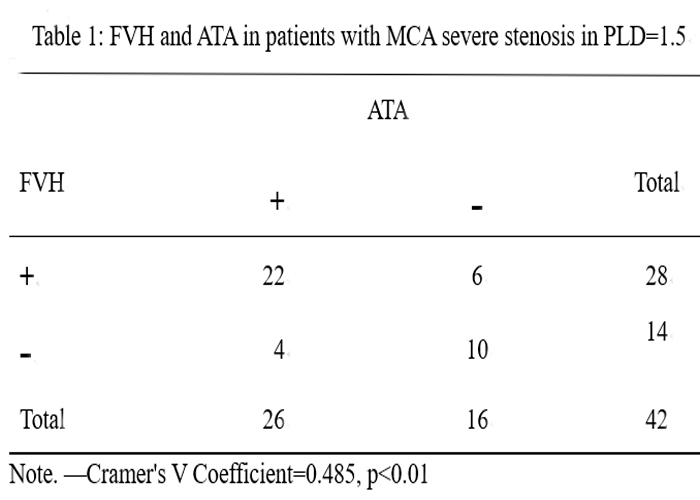
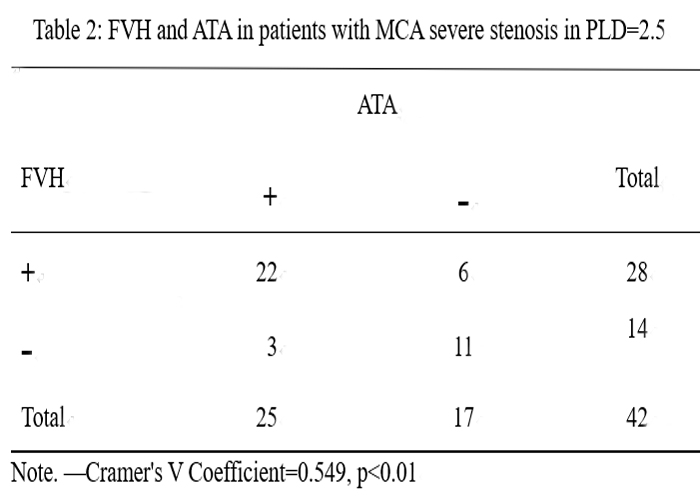
There were correlations between the FVH and occurrence frequency of ATA in affected lateral hemisphere in PLD = 1.5 s and PLD = 2.5 s, respectively (Cramer's V Coefficient=0.485, p<0.01; Cramer's V Coefficient=0.549, p<0.01, Figure1-2, Table1-2).Discussion
When the arterial arrival times are of the same scale or longer than PLD, labeled spins will be visualized in the arteries feeding the ischemic tissue, a finding that has been termed ATA1. One prior study suggested that patients with ATA had improved outcomes2, and that ATA may represent collateral flow. Some experiments prove that serpiginous ATA signal is disappeared on the vessel suppressed ASL images, confirming that the high signal is indeed vascular. FVH indicates the status of leptomeningeal collateral perfusion to vulnerable brain tissue. FVHs in patients are concerned with salvageable brain parenchyma3. Previous studies have focused on causes and clinical outcomes of both signs, and rarely on their relationship. Our experiments focuse on the relationship between FVH and ATA,because these two different sequences ( T2 FLAIR、3D ASL) can reflect collateral blood flow. In this study, we found that the appearance of FVH was correlated with the incidence of ATA, which further indicates that both signs are visual indicators for evaluating collateral flow. Moreover, the position of FVH and ATA is consistent. One likely explanation is that both of them are slow flow from the leptomeninx, which may be its etiology mechanism.Conclusion
The appearance of FVH has a good consistency with the occurrence and location of ATA in ASL imaging in patients with severe stenosis or occlusion in middle cerebral artery. The study has further confirmed the existence of collateral circulation.Acknowledgements
No acknowledgement found.References
1. Zaharchuk G. Arterial spin label imaging of acute ischemic stroke and transient ischemic attack.[J]. Neuroimaging Clin N Am, 2011, 21(2):285-301.
2. Chalela J A, Alsop D C, Gonzalez-Atavales J B, et al. Magnetic resonance perfusion imaging in acute ischemic stroke using continuous arterial spin labeling[J]. Stroke, 2000, 31(3):680-687.
3. Lee, S. H., et al. "Correlation between Hyperintense Vessels on FLAIR Imaging and Arterial Circulation Time on Cerebral Angiography. " Magnetic Resonance in Medical Sciences Mrms An Official Journal of Japan Society of Magnetic Resonance in Medicine 15.1(2015):124-128.
Figures