3254
Inner volume 3D TSE for isotropic 0.30 mm black-blood images of intracranial perforating arteries at 7T1State Key Laboratory of Brain and Cognitive Science, Beijing MR Center for Brain Research, Institute of Biophysics, Chinese Academy of Sciences, Beijing, China, 2University of Chinese Academy of Sciences, Beijing, China, 3Siemens Shenzhen Magnetic Resonance Ltd, Shenzhen, China, 4The Innovation Center of Excellence on Brain Science, Chinese Academy of Sciences, Beijing, China
Synopsis
The impairment of microvessels can lead to neurologic diseases such as stroke and vascular dementia. The imaging of lumen and vessel wall of perforating arteries requires an extremely high resolution due to their small caliber size (50 – 400 um). In this study, we developed a 3D inner-volume (IV) TSE (SPACE) sequence with 2D spatially selective excitation (SSE) RF pulses. High resolution of isotropic 0.30mm was achieved for the black-blood images of lenticulostriate artery (LSA) within 10 minutes. The IV-SPACE images showed clearer delineation of vessel wall and lumen of LSA than conventional SPACE images. IV-SPACE might be a promising method for detecting microvasculopathies of cerebral vascular diseases.
Introduction
The evaluation of perforating arteries (particularly the lenticulostriate artery, LSA) is important for
the diagnosis of small vessel disease1. However, there
is no suitable MRI imaging technique for both the lumen and vessel wall of perforating
arteries because of their small caliber size (50 – 400 um), which requires a high
spatial resolution. Inner volume (IV) imaging2 reduced field-of-view
(FOV) by using a multidimensional selective pulse3, enabling a high-resolution
image with small acquisition matrix to achieve an acceptable acquisition time.
In this study, 2D spatially selective excitation (SSE) RF pulses were used to
replace the excitation pulses of the conventional 3D turbo spin-echo (TSE, named SPACE by Siemens) sequence (IV-SPACE). The LSA lumen and vessel wall were
imaged by the IV-SPACE sequence with black-blood 0.30
mm isotropic resolution.Methods
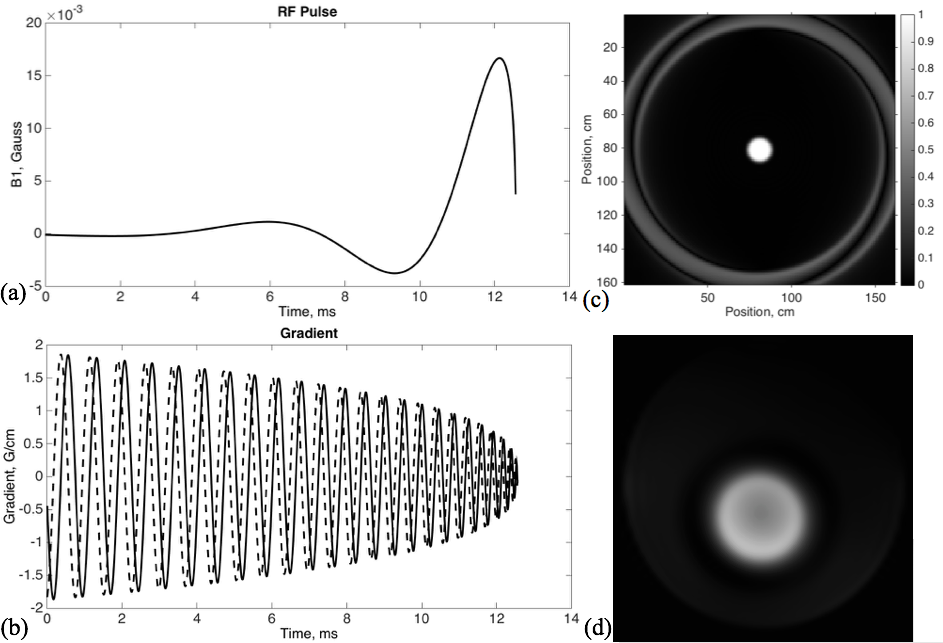
The 2D SSE pulse was designed with a spiral transmit
k-space trajectory, 24 turns, and a pulse length of 12.57 ms (Figure 1). The calculation
method was described in Pauly et al3 and
demonstrated the feasibility in subsequent literatures4. The disk diameter
was 5 cm, and the excitation FOV was 17 cm to avoid excitation aliasing.
A phantom scan was used to
verify the designed pulses by comparing the excitation profile with a simulated
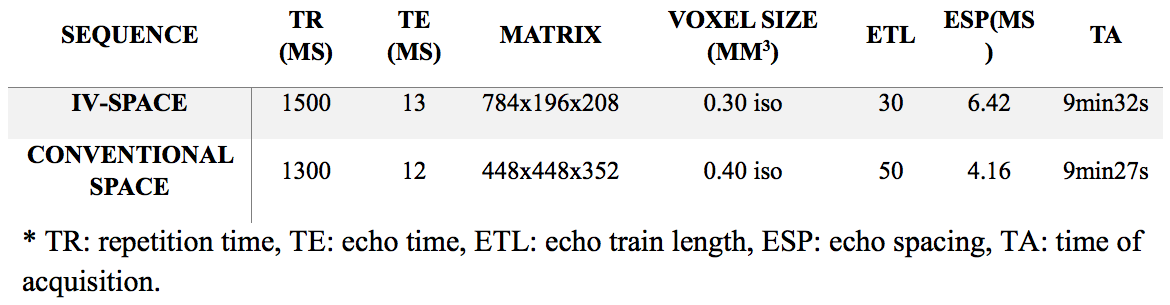
one. IV-SPACE with 0.30 mm isotropic
resolution and conventional SPACE with 0.40 mm isotropic resolution were used
for healthy volunteers, scanning on a 7T research system (Siemens Healthcare,
Erlangen, Germany) with a 1TX/32RX head coil. Key parameters are listed in
Table 1. The data of eight volunteers were
collected.Results
The phantom result of the excitation
profile is shown in Figure 1(d). It is consistent with the simulation in Figure
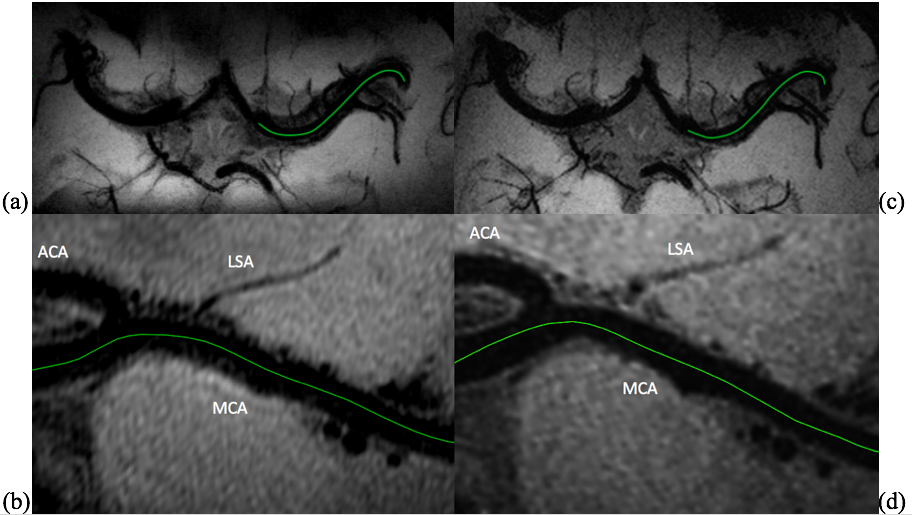
1(c). Examples of IV-SPACE and conventional SPACE images are
summarized in Figure 2. An axial minimum intensity projection (MinIP, slab thickness = 7.2 mm) and curved multiplanar reconstruction along the MCA are shown. The lumen and the orifice of an LSA are depicted in the IV-SPACE image, whereas it appears blurry in the conventional
SPACE image.
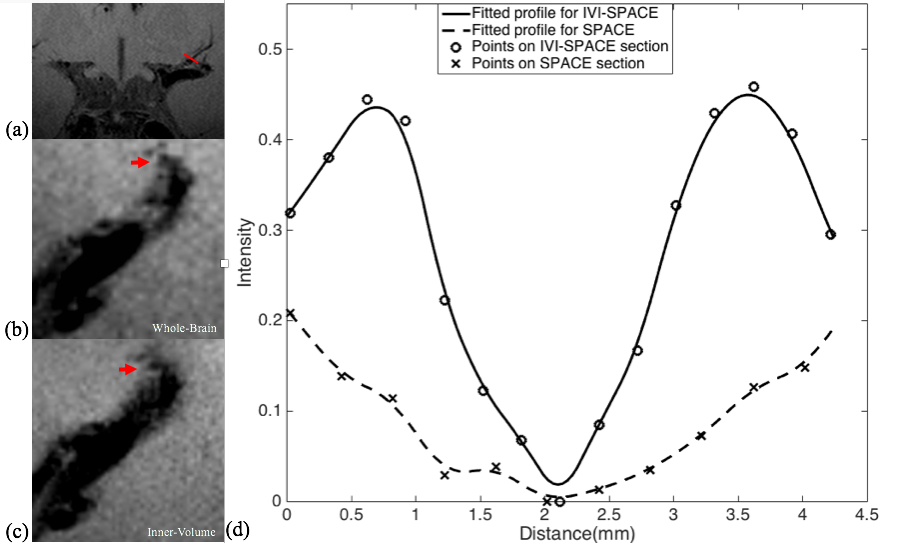
In Figure 3, the section view
of an LSA is shown and analyzed. The LSA vessel wall is obvious in IV-SPACE (red
arrow) but almost invisible in the conventional SPACE image. With a cut line though
the vessel center, IV-SPACE shows a significant signal drop at the lumen, which is almost absent in conventional
SPACE.
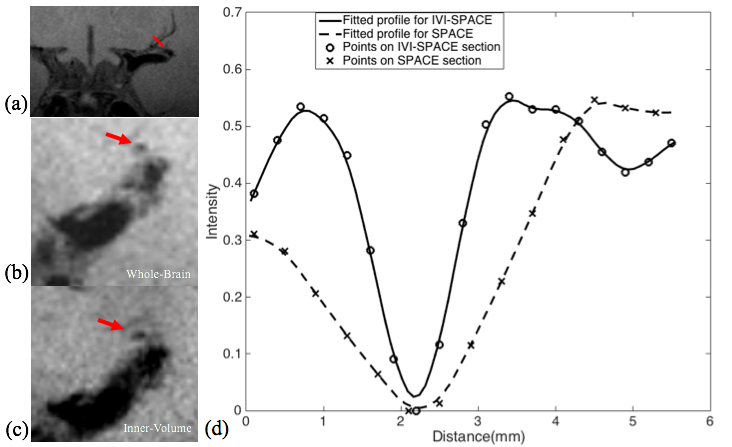
Figure
4 shows a case where the LSA wall is visible in both sequences; the IV-SPACE image has a higher contrast, and there is sharper delineation of the
vessel wall than in the conventional SPACE image.Discussion
Conventional SPACE uses non-selective pulse with
whole-brain coverage. Slab-selective SPACE reduces the matrix size only in the
head-foot direction. In contrast, the 2D SSE pulse reduces FOV in both the anterior-posterior
and head-foot directions. Therefore, IV-SPACE needs a smaller acquisition
matrix to cover MCA and LSA than conventional SPACE to achieve the same
resolution. IV-SPACE can be used to reduce acquisition times or have a higher
resolution. Moreover, the long and symmetric slab-selective pulse requires an
extra 180。pulse to prevent
stimulated echoes so that the arrival time of the first echo is prolonged and the
signal-to-noise ratio is decreased. However, the 180。pulse is not necessary for a spiral-in 2D SSE pulse,
which results in a stronger signal that is suitable for high-resolution
imaging.
This is the first time intracranial black-blood images with isotropic 0.30 mm resolution within ten minutes have
been demonstrated. The 2D SSE pulse is robust, and no obvious signal folding
from outer excitation FOV was observed, even though the B0 and B1+field
maps were not considered in the pulse design.
A higher spatial resolution reduces the partial
volume effect, so the LSA delineation is significantly improved in the
IV-SPACE images in Figure 2. The reduction of the echo train length from 50 to
30 might also contribute to sharpness of the vessel walls due to less signal decay (Figures 3 and 4). The sharper vessel wall potentially benefits the diagnosis and also the
study of cerebral vascular disease, such as the microvasculopathy in small
vessel disease, quantitative evaluation of the aneurysmal wall, and microstructure
of atherosclerotic plaques.
In our future research, B0
and B1+ field variations
should be incorporated into the pulse design, and better suppression of
aliasing should be optimized. Also, patients with cerebral vascular diseases
should be evaluated.Conclusion
The inner-volume 3D TSE sequence was developed to
achieve isotropic 0.30 mm black-blood images within a clinically acceptable
time. A higher resolution produces sharper delineation of the vessel wall and
lumen of intracranial perforating arteries. The technique is promising for the
evaluation of microvasculopathies of cerebral vascular diseases.Acknowledgements
This work was supported in part by the Beijing Municipal Natural Science Foundation (7184226), Young Elite Scientists Sponsorship Program by CAST (2017QNRC001), Ministry of Science and Technology of China grant (2015CB351701), and the Chinese Academy of Sciences grant (XDBS01000000).References
1. Greenberg, S.M., Small vessels, big problems. N Engl J Med, 2006. 354(14): p. 1451-3.
2. Feinberg D A, Hoenninger J C, Crooks L E, et al. Inner volume MR imaging: technical concepts and their application[J]. Radiology, 1985, 156(3): 743-747.
3. Pauly J, Nishimura D, Macovski A. A k-space analysis of small-tip- angle excitation. J Magn Reson 1989;81:43–56.
4. Mitsouras D, Mulkern RV, Rybicki FJ. Strategies for inner volume 3D fast spin echo magnetic resonance imaging using nonselective refocusing radio frequency pulses. Med. Phys. 2006; 33: 173–186.
Figures