3251
Comparison of cerebrovascular reactivity among patients with sporadic cerebral small vessel disease1Graduate Institute of Mind, Brain and Consciousness, Taipei, Taiwan, 2Department of Neurology, Stroke Center, Chang Gung Memorial Hospital, Linkou Medical Center, Taoyuan, Taiwan
Synopsis
Sporadic cerebral small vessel disease (SVD) affects small vessels in the brain and causes cerebrovascular-event-related disability. We separated patients into two groups (acute ischemic stroke and spontaneous intracranial hemorrhage) and then compared their cerebrovascular reactivity (CVR) with normal control. We found there was significant BOLD amplitude decline between normal and ischemic group, but no difference in the temporal estimates between groups.
Introduction
Cerebral small vessel disease (SVD), a group of pathological processes in the brain that affect the small vessels[1], potentially causes cerebrovascular-related episodes such as cognitive, physical disabilities or dementias.[2] Cerebrovascular reactivity (CVR) was reported to be a sensitive method to evaluate hemodynamics in patients with carotid stenosis or other stoke patients in former study.[3, 4] However, CVR between different stereotypes of acute SVD patients, such as acute ischemic stroke and spontaneous intracranial hemorrhage, remain unknown. We hypothesized that SVD patient groups show distinct CVR outcomes in both strength and temporal characteristics. Methods
Forty
recruited patients were divided into three groups, normal control (age:61.1±5.2,
3 males of 7), acute ischemic stroke (age:61.0±9.67, 16 males of 25) and acute
spontaneous intracranial hemorrhage (age:55.0±11.2, 7 males of 8). The patients
received MRI assessments at the acute phase (<10 days from onset) of stroke at
a 3T Discovery MR750. During the CVR scanning with GE-EPI BOLD sequence
(TR/TE=3000/35 ms, voxel size=3.4×3.4×3.5 mm, 40 slices, Flip angle=90°, 100
measurements), we performed a block-designed CO2 inhalation paradigm
of alternating air and hypercapnic gas mixture (CO2 7% balanced with
air). We used the processing steps of CVR calculation in IClinfMRI[5] for individual and group analysis. Temporal features (such as onset time,
time-to-peak, etc) were generated using the dual-gamma fitting to the averaged
BOLD response of CO2 inhalation for each individual. At last we performed
group comparisons with using one-way ANOVA.Results
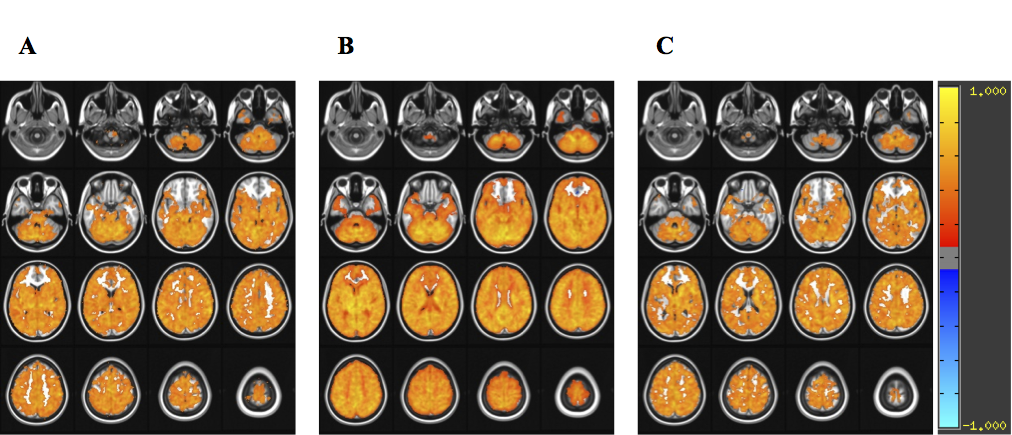
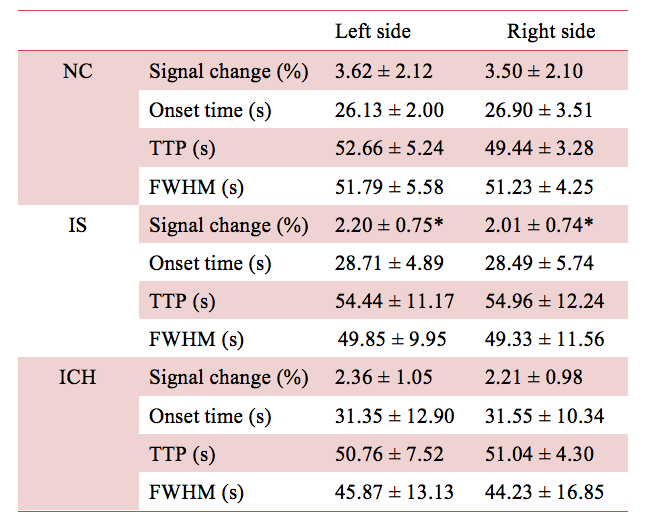
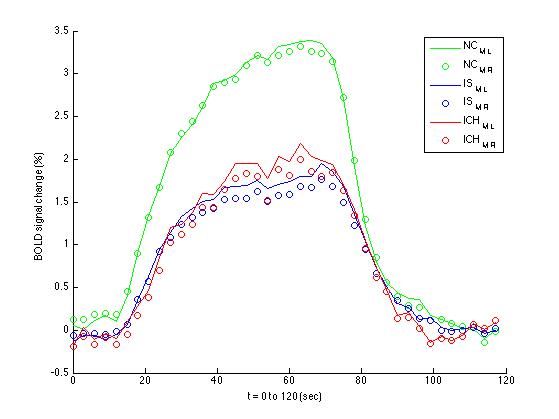
In BOLD-fMRI, the CVR map for each group (Fig. 1) were presented. Based on Automated Anatomical Labeling (AAL), we extracted the ROI (19, 20; Supp_Motor_Area, L& R) and exerted curve fitting to calculate the temporal parameters (Table 1). Though no apparent disparity in the temporal parameters was found among three groups, the BOLD amplitude of the ischemic group was significantly reduced in contrast to that of the control group (Table 1). Figure 2 further illustrates the averaged hemodynamic response in left and right ROIs for each group (Fig. 2).Discussion and Conclusion
In this preliminary research, we examined whether CVR possessed the sensitivity to the heterogeneity across different SVD causes. No apparent conclusion could be achieved using temporal parameters. One of the limitations was the heterogeneity of lesion sides, potentially affects the expression of temporal parameters. However, we found a significant amplitude reduction between normal control and the ischemic group (marginal significance for the hemorrhage group), which was relatively sensitive to the patients with carotid stenosis.Acknowledgements
We thank the Magnetic Resonance Imaging Center of Linkou Chang Gung Memorial Hospital for their kind support in imaging arrangement. Funding This study was carried out under the grants from the Ministry of Science and Technology, Taiwan (Grants MOST 107-2314-B-182A-053 -).References
[1.] Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010; 9:689–701.
[2.] Wardlaw JM, Smith C, Dichgans M. Mechanisms underlying sporadic cerebral small vessel disease: Insights from neuroimaging. The Lancet Neurology. 2013;12:483-497
[3.] Chang TY, Kuan WC, Huang KL, Chang CH, Chang YJ, Wong HF, et al. Heterogeneous cerebral vasoreactivity dynamics in patients with carotid stenosis. PLoS One. 2013;8:e76072
[4.] Thrippleton et al. Cerebrovascular reactivity measurement in cerebral small vessel disease: Rationale and reproducibility of a protocol for MRI acquisition and image processing, Int J Stroke. 2018 Feb;13(2):195-206.
[5.] Hsu et al., IClinfMRI Software for Integrating Functional MRI Techniques in Presurgical Mapping and Clinical Studies. Frontiers in Neuroinformatics. 2018 ;(12)
Figures