3243
Intracranial Vessel Wall Imaging: Artifactual Effects of Localized Movement and In-line Mitigation with Self-gating1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Bioengineering, University of California, Los Angeles, CA, United States, 3Siemens Healthcare, Los Angeles, CA, United States, 4Department of Radiology, Xuanwu Hospital, Beijing, China, 5Department of Neurology, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 6Department of Imaging, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 7Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 8Department of Medicine, University of California, Los Angeles, CA, United States
Synopsis
Intracranial vessel wall imaging can directly visualize the vessel wall and characterize wall
Introduction
Intracranial vessel wall imaging (VWI) can directly visualize the vessel wall and characterize wall pathologies, and has drawn great clinical interest1. 3D variable-flip-angle turbo spin-echo (aka. SPACE, VISTA, or CUBE) is currently the method of choice for intracranial VWI. However, because of its 3D acquisition fashion, this method is inherently susceptible to motion as previously shown in extracranial VWI studies2. For intracranial VWI, motion may also result from bulk or localized (coughing and swallowing) movement, although the former can be effectively reduced by using foam pads. Reducing motion degradation becomes more critical because of long scan time (7-12 min) and demanding spatial resolution (0.5 mm). This work aims to investigate the effect of localized movement on intracranial VWI quality and to present an in-line self-gating (SG) approach to mitigate quality deterioration.Methods
Technique
We developed a self-gated SPACE (SG-SPACE) imaging technique. Specifically, a commercially available T1-weighted SPACE sequence was modified as follows. A center k-space line (i.e. SG line), in the superior-inferior direction, is acquired from the first echo of the SPACE readout. The projection of the entire imaging volume is derived by the Fourier transform of the SG line. The projections acquired in subsequent repetition time (TR) periods are cross-correlated (CC) to the reference projection that is collected at the beginning. All acquired TRs are prioritized based on the severity of motion contamination as indicated by their CC values, and the most affected TRs are reacquired at the end of scan and used for on-line reconstruction. The number of allowed reacquisitions can be set through the user-interface, and thus the scan time remains fixed.
In vivo Studies
Eight healthy volunteers were recruited in the study with informed consent. All scans were performed on a 3T system (MAGNETOM Skyra; Siemens Healthineers, Germany) equipped with a 20-channel head-neck coil. All subjects underwent three vessel wall scans using the developed SG-SPACE technique: (a) imaging with the SG function off and without motion instructions (denoted as “No Motion”); (b) imaging with the SG function on and with coughing instructions; and (c) imaging with the SG function on and with swallow instructions. In addition to the online-reconstructed images (denoted as “With MOCO”) from the latter two scans, their raw data were also used to reconstruct motion-contaminated images (denoted as “Without MOCO”) by retrospectively retrieving the data acquired in motion-corrupted TRs. Motion instructions were given over the intercom system at five preset stages. The imaging protocol recently presented for whole-brain VWI3 was used in all scans: sagittal orientation, TR/TE = 900/10 ms, 0.53 mm isotropic resolution, 8 min acquisition time without motion or SG. The number of reacquisition TRs was 30 when SG was enabled.
Data Analysis
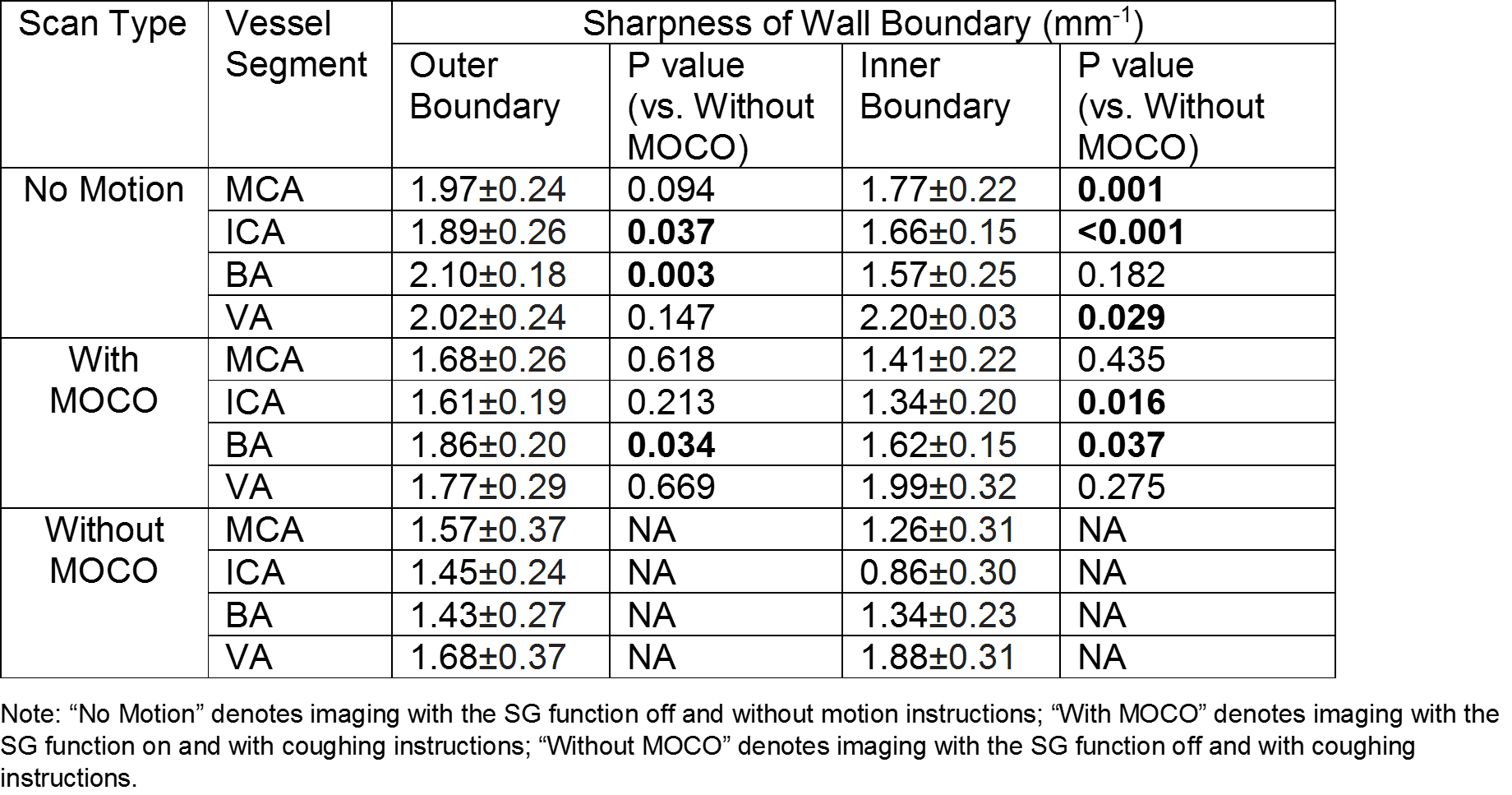
To quantify the effect of motion on image quality and the effectiveness of SG in preventing quality deterioration, vessel wall sharpness was measured at the inner and outer boundaries of 4 major vessel segments including middle cerebral arteries (MCA), internal carotid arteries (ICA), basilar arteries (BA) and vertebral arteries (VA). Reformatted 2D cross-sectional images were used for the purpose using our in-lab MATLAB program2. The paired two-tailed Student’s t test was used for the comparison of sharpness between scans.
Results
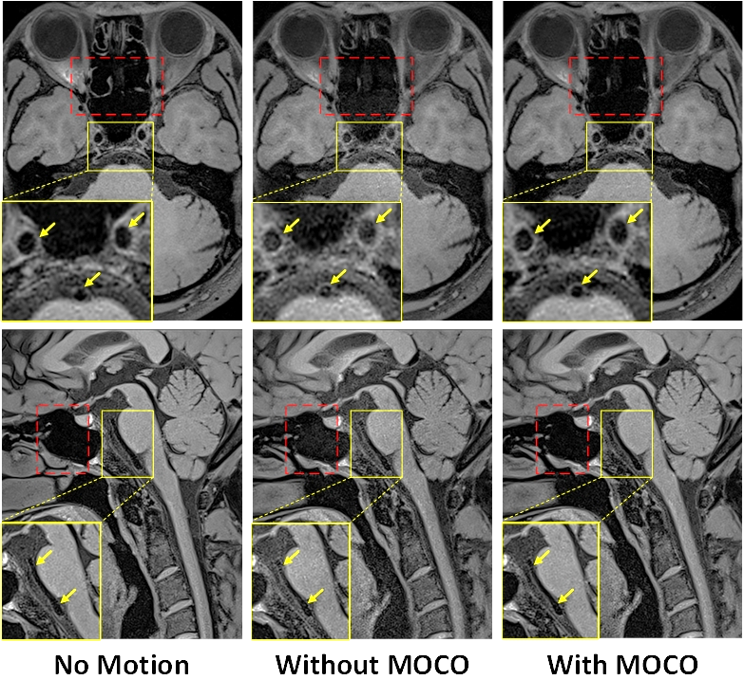
In general, coughing and swallowing motion resulted in noticeable blurring and noise at the vessels in close proximity to the nasal and oral cavities (Figure 1-3). These artifacts were well suppressed by reacquiring motion corrupted k-space lines detected by SG signals. For scans with coughing instructions, representative time-courses of projection profiles and CC-values are shown in Figure 4, suggesting that motion events were reliably detected. As shown in Table 1, coughing significantly reduced vessel wall sharpness at either outer or inner vessel wall boundary (check p values for “No Motion” vs. “Without MOCO”), particularly at the ICA and BA. The use of in-line SG significantly mitigated the effect at both vessels (check p values for “With MOCO” vs. “Without MOCO”).Discussion
While underexplored to date, likely because 3D intracranial VWI has become a hot research topic since 20114, motion susceptibility could critically undermine VWI’s clinical translation. This is the first study demonstrating that localized movement of internal anatomic structures due to coughing and swallowing can cause severe motion artifacts and significantly impair vessel wall delineation. The SG motion compensation approach can significantly mitigate the above problems. This technical improvement may potentially be useful for improving success rate of such scans and ensuring accurate assessment of vessel wall pathologies.Conclusion
Localized movement can induce substantial artifactual effect in intracranial VWI, and in-line mitigation with self-gating is feasible.Acknowledgements
No acknowledgement found.References
1 Mandell DM, Mossa-Basha M, Qiao Y, et al. Intracranial vessel wall MRI: principles and expert consensus recommendations of the American Society of Neuroradiology. AJNR Am J Neuroradiol. 2017;38(2):218 –29.
2 Fan Z, Zuehlsdorff S, Liu X, et al. Prospective self-gating for swallowing motion: a feasibility study in carotid artery wall MRI using three-dimensional variable-flip-angle turbo spin-echo. Magn Reson Med. 2012;67:490-8.
3 Yang Q, Deng Z, Bi X, et al. Whole-brain vessel wall MRI: a parameter tune-up solution to improve the scan efficiency of three-dimensional variable-flip-angle turbo spin-echo. J Magn Reson Imaging. 2017;46:751-57.
4 Qiao Y, Steinman DA, Qin Q, et al. Intracranial arterial wall imaging using three-dimensional high isotropic resolution black blood MRI at 3.0 tesla. J Magn Reson Imaging. 2011;34:22–30.
Figures