3241
Assessment of intracranial atherosclerotic plaques using 3D non-contrast black blood MRI: comparison with DSA1Radiology, Changhai hospital, Shanghai, China, 2Radiology and Biomedical imaging, University of California, San Francisco, CA, United States
Synopsis
Digital subtraction angiography (DSA) remains the gold standard for assessment of intracranial artery stenosis. However, it is invasive and may miss lesions without luminal stenosis due to vessel wall outward remodeling. We compared 3D black-blood MRI (SPACE) with DSA in 74 intracranial plaques, and found SPACE was in good agreement with DSA for stenosis quantification (ICC=0.82), but the plaque was longer in SPACE than DSA. Moreover, SPACE detected 28 more plaques than DSA, and 14 of 28 plaques showed enhancement. SPACE is promising for evaluating the severity of intracranial atherosclerosis and may improve patient management.
Purpose:
Digital subtraction angiography (DSA) remains the gold standard for assessment of intracranial artery stenosis. However, this invasive procedure is known to have certain limitations, including radiation exposure and difficulty in visualizing potentially high-risk lesions without luminal stenosis due to vessel wall outward remodeling. Previous studies showed plaque could present in non-stenotic basilar artery and predicted unfavorable functional outcome after 3 months1. However, the comparison between SPACE and DSA for intracranial artery plaque assessment is still very limited. Our study aims to assess 3D non-contrast black-blood MRI as a noninvasive alternative approach to DSA for evaluating intracranial stenosis.Methods:
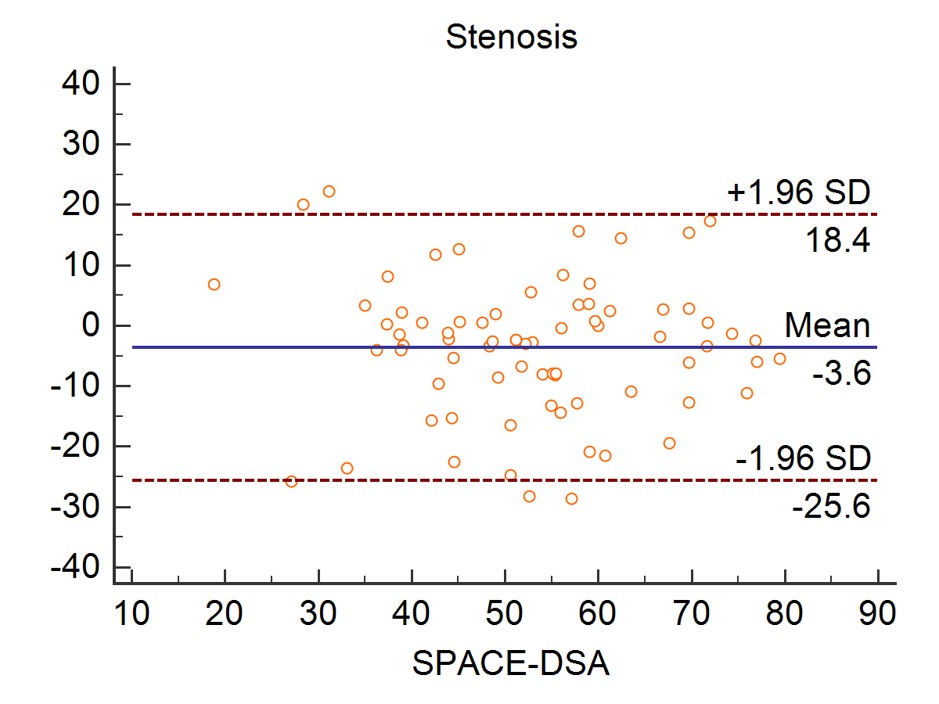
Study population: 42 symptomatic patients (mean age, 62.3±9.1 years, 35 males) with 102 intracranial atherosclerotic plaques were included in the analysis. All patients were scanned in a Siemens 3T scanner (Skyra) using the standard head coil. Imaging protocol: 1) 3D black blood SPACE (variable flip angle fast-spin-echo 2) acquired in sagittal plane, 0.5mm isotropic resolution, echo train length 60, TR/TE = 900/5.6ms, scan time 8’16”. 2) 3D rotational DSA was acquired following clinical protocol with a 5-second rotation of 200° (144 frames), FOV 32cm and matrix 1024, resulting in 0.3mm in-plane resolution. Image analysis: Luminal stenosis was measured on both DSA and SPACE by a reviewer blinded to the patient information. On a subset of SPACE images (n=20), another reviewer measured the stenosis value independently for the evaluation of reproducibility. Plaque enhancement and maximal plaque thickness were recorded. Bland Altman plots were used when comparing SPACE with DSA for stenosis quantification.Results:
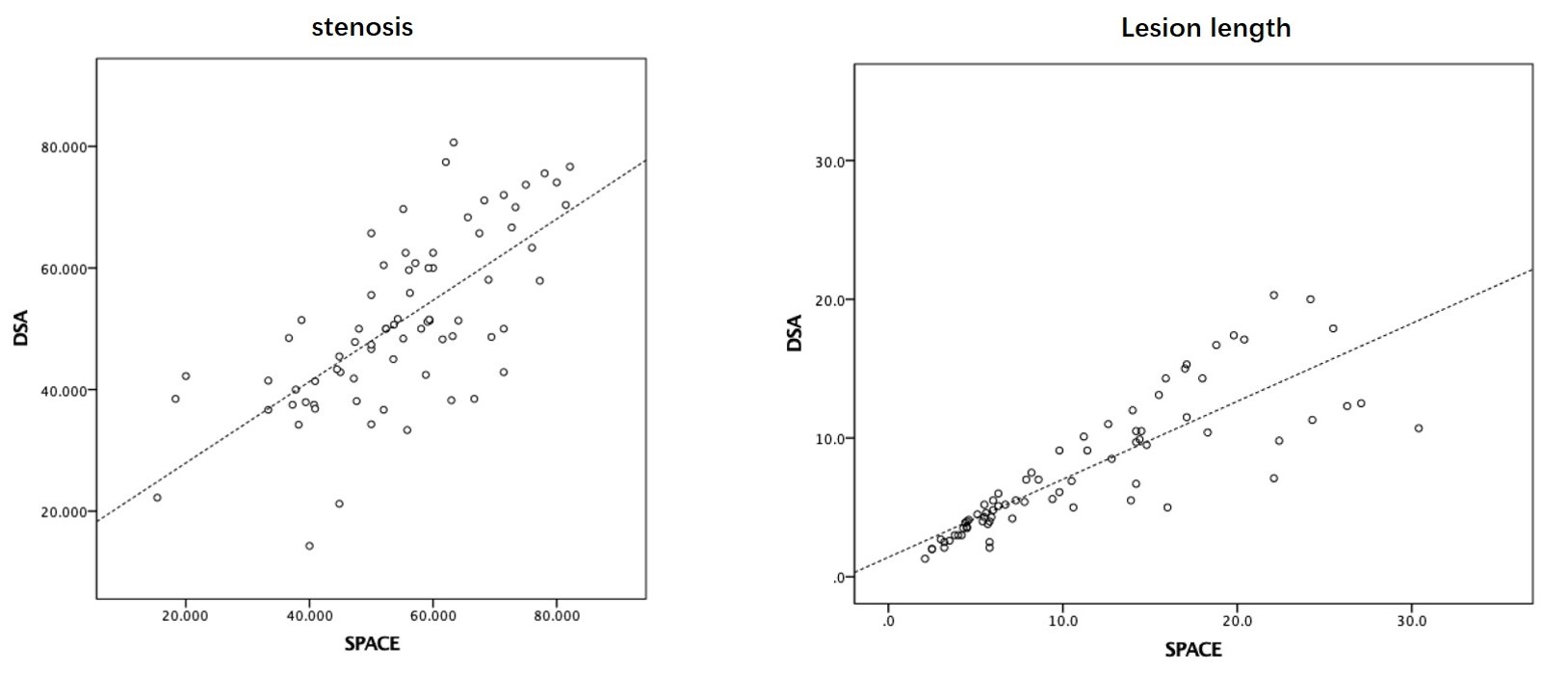
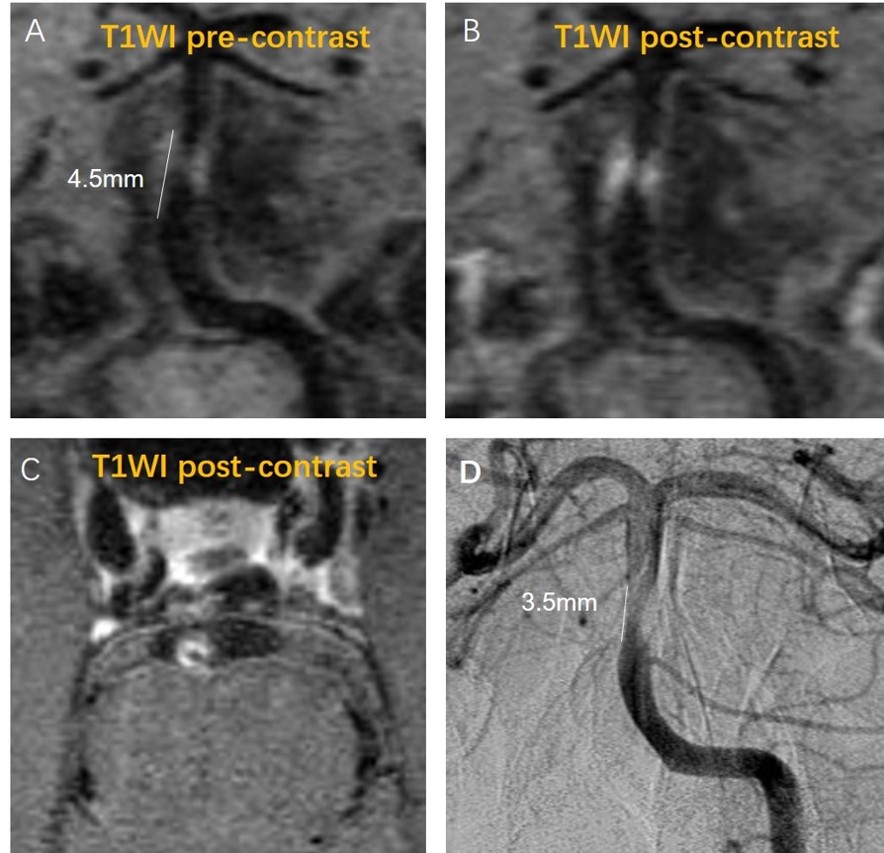
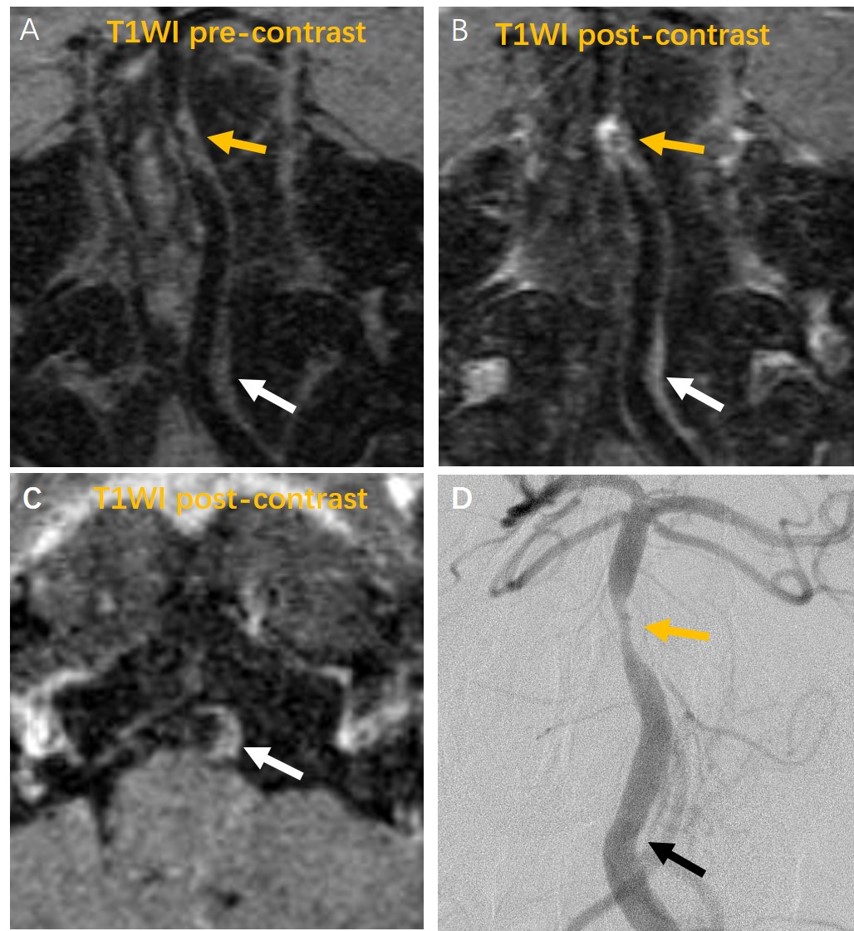
Patient demographic information was summarized in Table 1. SPACE revealed 102 plaques, while DSA revealed 74 plaques. 28 plaques (27.4%) were stenosis-free on DSA, but were shown clearly on SPACE. Good agreement in measuring stenosis was found between SPACE and DSA (ICC = 0.82, Figure 1). Figure 2 showed that there was significant correlation between SPACE and DSA in measuring stenosis and in lesion length. However, lesion length measurements by using SPACE were longer than those measured by using DSA (11.1±7.2mm vs. 7.7±4.8mm, P<0.001). Sample images were shown in Figure 3-4. Of the 28 non-stenotic plaques, 14 were shown contrast enhancement (Figure 4). The maximal wall thickness of those 28 plaques was 0.86±0.25mm (range 0.5 to 1.3mm). There was excellent inter-reader agreement for measuring the degree of stenosis (ICC = 0.99) and for lesion length (ICC = 0.99) on SPACE images by two readers.Discussion:
To our knowledge, this is the first study comparing SPACE and DSA for both intracranial plaque detection and stenosis quantification. We found 3D black-blood MRI showed high agreement with DSA for stenosis measurements, in line with previous studies2. In addition, SPACE depicted a longer lesion length than DSA because of outward remodeling, also in agreement with previous reports on carotid plaque3. Our results support the use of non-contrast SPACE as an alternative way for quantifying intracranial stenosis, and SPACE provides better description of plaque length. More importantly, more than 1/4 of plaques shown on SPACE were invisible on DSA, however such plaque can cause ischemic events1,4. SPACE also allows the characterization of novel imaging markers for vulnerable plaque, including intra-plaque hemorrhage and enhancement5. Because SPACE can detect significantly more lesions and provide novel imaging markers, it has great potential to improve the risk stratification of patients with intracranial plaque.Conclusion:
3D black-blood MRI is accurate and reproduceable for quantifying intracranial artery stenosis comparing with DSA. It also detects more plaques, which may improve current patient management strategy.Acknowledgements
I am greatly indebted to my supervisor, Professor Jianping Lu, for his valuable instructions and suggestions on my thesis. Grateful acknowledgement is also made to Professor Chengcheng Zhu who gave me considerable help by means of suggestion, comments and criticism. In addition, I deeply appreciate the contribution to this thesis made in various ways by my friends, workmates and my husband.
References
1. Cho HJ, Kim KH, Kim EJ, et al. Clinical Implications of Basilar Artery Plaques in the Pontine Infarction with Normal Basilar Angiogram: A High-Resolution Magnetic Resonance Imaging Study. Journal of Stroke and Cerebrovascular Diseases, 2018.
2. Park JE, Jung SC, Lee SH, et al. Comparison of 3D magnetic resonance imaging and digital subtraction angiography for intracranial artery stenosis. Eur Radiol, 2017; 27(11): 4737-4746.
3. Zhao H, Wang J, Liu X, et al. Assessment of carotid artery atherosclerotic disease by using three-dimensional fast black-blood MR imaging: comparison with DSA. Radiology, 2015; 274(2): 508-16.
4. Harteveld AA, Denswil NP, Van HW, et al. Ex vivo vessel wall thickness measurements of the human circle of Willis using 7T MRI. Atherosclerosis, 2018; 273: 106-114.
5. Zhu CC, Tian X, Degnan AJ, et al. Clinical Significance of Intraplaque Hemorrhage in Low- and High-Grade Basilar Artery Stenosis on High-Resolution MRI. AJNR Am J Neuroradiol, 2018; 39(7): 1286-1292.
Figures
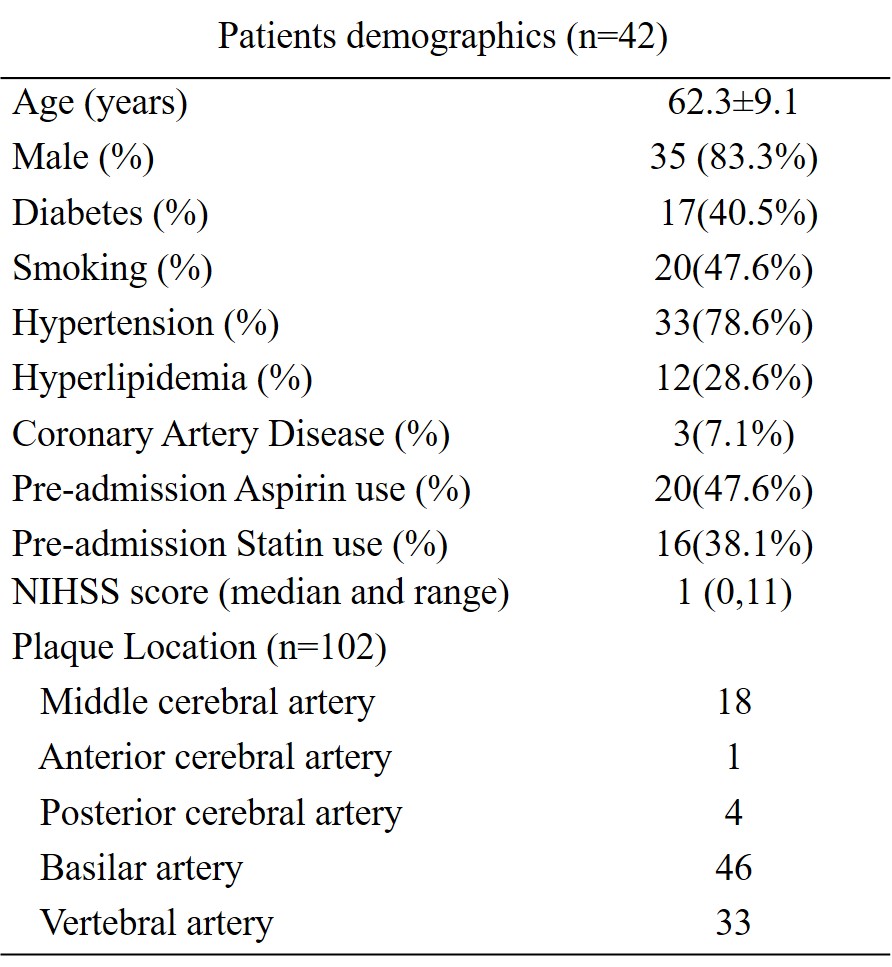
Table 1. Patients demographics.
NIHSS: National Institutes of Health Stroke Scale