3232
Evaluation of Neuroprotective Effects of Cyclosporine in a Porcine Model of Focal Traumatic Brain Injury using Diffusion Tensor Imaging1Department of Anesthesiology and Critical Care, Children's Hospital of Philadelphia, Philadelphia, PA, United States, 2Neurovive Pharmacuetical AB, Lund, Sweden, 3Mitochondrial Medicine, Department of Clinical Sciences, Lund University, Lund, Sweden, 4Department of Neurosurgery, Rigshospitalet, Copenhagen, Denmark, 5Department of Radiology, Perelman School of Medicine at University of Pennsylvania, Philadelphia, PA, United States
Synopsis
A moderate focal contusion injury model in swine was used to evaluate treatment response to cyclosporine, a neuroprotective agent, using diffusion tensor imaging. This work builds upon the recent work in which we demonstrated improved neurological outcomes after administration of cyclosporine in the acute time period following traumatic brain injury (TBI). Regions of interests were drawn on the peri-contusion regions. We observed significant elevations in FA and CL and significant decline in CS from cyclosporine groups compared to those of placebo. These findings suggest that DTI may be useful in assessing treatment response to cyclosporine in a porcine model of TBI.
Introduction
Traumatic brain injury (TBI) is a leading cause of death and long-term disability worldwide.1 TBI is caused by physical trauma to the head or a rapid acceleration-deceleration process.2 After the primary injury associated with immediate structural damage, mitochondrial dysfunction and oxidative tissue damage are the secondary events that continue to evolve in TBI.3 Cyclosporine has multiple mechanisms of action that can be beneficial for treating TBI.4 Recently,5 we reported the positive treatment effects of a novel formulation of cyclosporine (a neuroprotective agent) in a porcine model of focal TBI. Cyclosporine significantly reduced the volume of parenchymal injury and improved markers of neuronal injury, as measured with magnetic resonance spectroscopy. Additionally, positive improvements in brain metabolism and mitochondrial function were observed in the peri-contusional tissues. Diffusion tensor imaging (DTI) is an advanced magnetic resonance imaging technique that is capable of providing rich information on the brain's cytoarchitectural integrity.6,7 Several studies have shown the potential of DTI to understand the pathophysiology of TBI8,9 and to evaluate the treatment response to therapeutic agents.10-12 The purpose of current study was to investigate the potential utility of DTI in evaluating treatment efficacy of cyclosporine in a randomized, blinded preclinical trial involving a porcine model of focal TBI.Methods
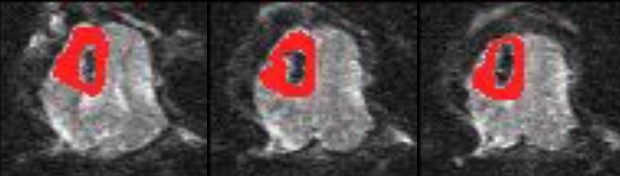
A moderate focal contusion injury was induced in piglets using a controlled cortical impact device. After initial step-wise analyses of pharmacokinetics, a 5-day dosing regimen with continuous intravenous infusion using a cremophore-free lipid emulsion formulation of cyclosporine (NeuroSTAT®, 20 mg/kg/day) was evaluated in a randomized and blinded placebo-controlled setting. A total of 24 animals received the full dose (n = 11 with cyclosporine and n = 13 with matching placebo). All these animals underwent anatomical imaging and DTI besides other sequences on a 3T MR system. DTI data were acquired using 30 directions with a single-shot spin-echo, echo-planar sequence with parallel imaging. The sequence parameters included: TR/TE=5,000/86ms, NEX=3, FOV=22×22cm2, matrix size=128×128, in-plane resolution=1.72×1.72mm2; slice thickness=3mm; b = 0, 1,000s/mm2, number of slices=40. Of these 24 animals, data from 4 animals was incomplete or corrupted and hence these 4 animals were excluded. As a result, the final data analysis included two groups of animals [cyclosporine (n=8) and placebo (n=12)]. The artifacts induced by eddy currents and/or subject motion were minimized using an IDL based in-house developed algorithm.13,14 Pixel-wise parametric maps of mean diffusivity (MD), fractional anisotropy (FA), coefficient of linear (CL), planar (CP) and spherical (CS) anisotropy maps were generated. A 3D composite mask was drawn on the hyperintense peri-contusion tissue regions carefully avoiding the hypointense hemorrhagic components encompassing all slices of b0 image (Figure 1). A similar composite mask was drawn on the contralateral normal brain parenchyma. The mean values of DTI metrics (MD, FA, CL, CP and CS) were computed from peri-contusion tissues and were normalized with respect to contralateral normal brain parenchyma in each case. These normalized parameters were compared between placebo and treatment groups using unpaired t-tests. A probability (p) of 0.05 was considered significant. Additionally, receiver operating characteristic (ROC) curve analyses were used to determine accuracy (area under the ROC curve) associated with each parameter.Results
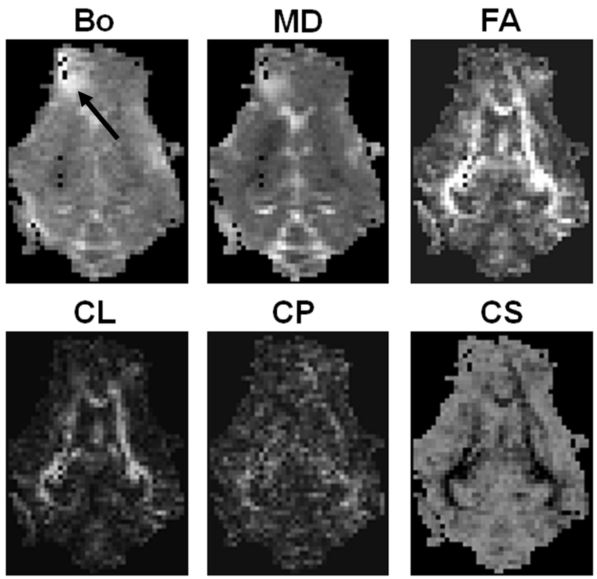
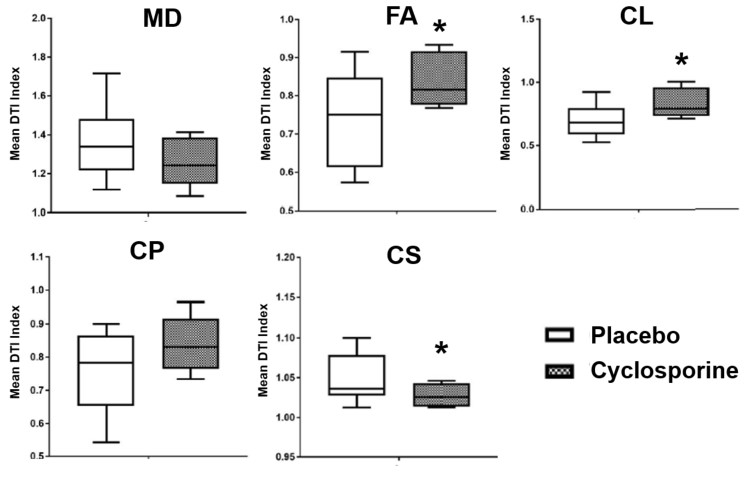
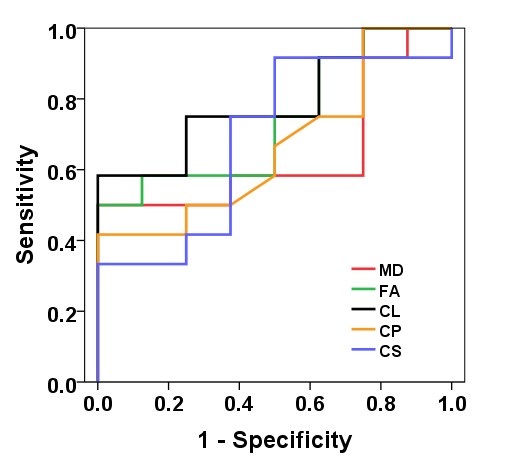
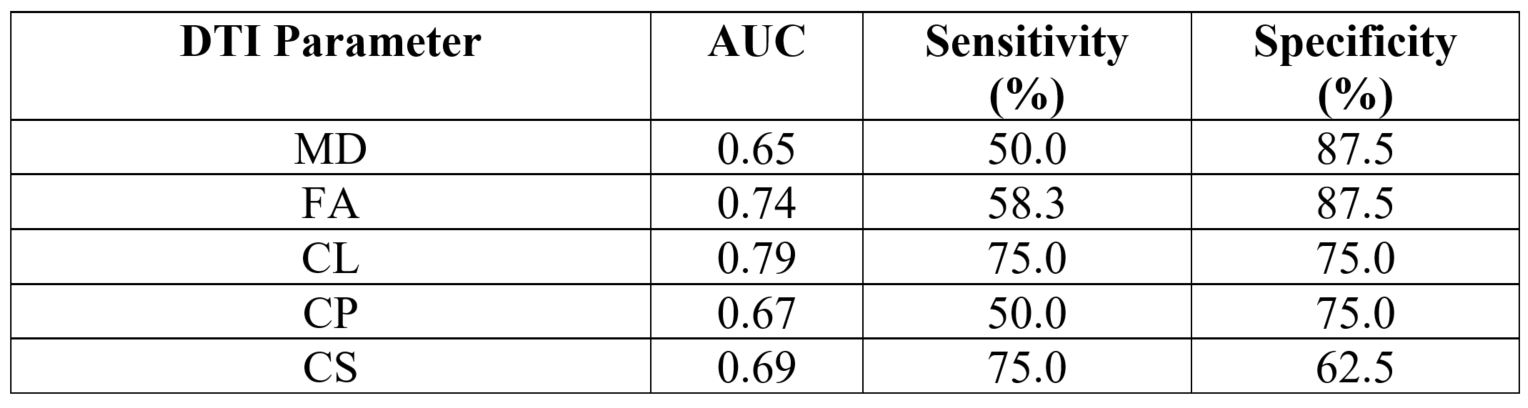
Representative DTI maps from cyclosporine group are shown in Figure 2. The distributions of DTI indices between placebo and cyclosporine treatment groups are presented as box and whisker plots (Fig. 3). Significant elevations in normalized FA (0.74± 0.12 vs. 0.84± 0.07, p=0.027) and normalized CL (0.69± 0.13 vs. 0.83± 0.11, p=0.018) and significant decline in normalized CS (1.07± 0.03 vs. 1.02± 0.01, p=0.042) were observed from cyclosporine groups compared to those of placebo. There were no significant differences (p>0.05) in MD and CP between two groups. ROC analyses demonstrated that CL had the best accuracy (0.79) in distinguishing placebo from treatment groups with a sensitivity of 75.0% and a specificity of 75.0% (Fig. 4). A summary of sensitivity and specificity for different DTI parameters in distinguishing placebo from cyclosporine treated groups is presented in Table 1.Conclusion
Our data suggest that DTI may be an imaging modality for neurotherapeutic evaluation in TBI. Specifically, our findings indicate that potential efficacy of the neuro-reparative agent cyclosporine in promoting recovery may be tested using DTI derived parameters as surrogates for structural and functional outcomes.Acknowledgements
No acknowledgement found.References
1. Marin JR, Weaver MD, Yealy DM, et al. Trends in visits for traumatic brain injury to emergency departments in the United States. JAMA. 2014;311:1917-1919.
2. Hawryluk GW, Bullock MR. Past, present, and future of Traumatic Brain Injury research. Neurosurg Clin N Am. 2016;27:375-396.
3. Robertson CL, Scafidi S, McKenna MC, et al. Mitochondrial mechanisms of cell death and neuroprotection in pediatric ischemic and traumatic brain injury. Exp. Neurol. 2009;218,371-380.
4. Hansson, M.J., Mansson, R., Mattiasson, G., et al. Brain-derived respiring mitochondria exhibit homogeneous, complete and cyclosporin-sensitive permeability transition. J. Neurochem. 2004;89,715-729.
5. Karlsson M, Pukenas B, Chawla S, et al. Neuroprotective Effects of Cyclosporine in a Porcine Pre-Clinical Trial of Focal Traumatic Brain Injury. J Neurotrauma. 2018 Jul 24. doi: 10.1089/neu.2018.5706.
6. Le Bihan D, Johansen-Berg H. Diffusion MRI at 25: exploring brain tissue structure and function. Neuroimage 2012;61:324-341.
7. Oishi K, Faria AV, Yoshida S, et al. Quantitative evaluation of brain development using anatomical MRI and diffusion tensor imaging. Int J Dev Neurosci. 2013;31(7):512-524.
8. Wortzel HS, Kraus MF, Filley CM, et al. Diffusion tensor imaging in mild traumatic brain injury litigation. J Am Acad Psychiatry Law. 2011;39(4):511-523.
9. Sharp DJ, Ham TE. Investigating white matter injury after mild traumatic brain injury. Curr Opin Neurol. 2011;24(6):558-563.
10. Robinson S, Winer JL, Chan LAS, et al. Extended Erythropoietin Treatment Prevents Chronic Executive Functional and Microstructural Deficits Following Early Severe Traumatic Brain Injury in Rats. Front Neurol. 2018;9:451. doi: 10.3389/fneur.2018.00451.
11. Strangman GE, O'Neil-Pirozzi TM, et al. Fractional anisotropy helps predicts memory rehabilitation outcome after traumatic brain injury. NeuroRehabilitation. 2012;31(3):295-310.
12. Robinson S, Winer JL, Berkner J, et al. Imaging and serum biomarkers reflecting the functional efficacy of extended erythropoietin treatment in rats following infantile traumatic brain injury. J Neurosurg Pediatr. 2016;17(6):739-755.
13. Wang S, Kim S, Chawla S, et al. Differentiation between glioblastomas and solitary brain metastases using diffusion tensor imaging. Neuroimage 2009;44:653-660.
14. Chawla S, Wang S, Mohan S, et al. Differentiation of brain infection from necrotic glioblastoma using combined analysis of diffusion and perfusion MRI. J Magn Reson Imaging. 2018 Apr 20. doi: 10.1002/jmri.26053.
Figures