3231
Improvements in specificity by non-Gaussian diffusion modeling and double diffusion encoding (DDE) to characterize axonal injury1NIBIB, NIH, Bethesda, MD, United States, 2Henry M. Jackson Foundation, Inc, Bethesda, MD, United States, 3NICHD, NIH, Bethesda, MD, United States
Synopsis
Diffusion MRI techniques that extend beyond diffusion tensor imaging (DTI) – including acquisition strategies and advanced modeling – could provide more specific tools to probe abnormalities in disease or injury states. To evaluate similarities and distinctions across several prominent diffusion MRI strategies in the context of injury, we acquired multi-shell diffusion weighted images (DWIs) and double diffusion encoded (DDE) DWIs in healthy and injured ferret spinal cords. Scalar metrics from DTI, diffusion kurtosis imaging (DKI), mean apparent propagator MRI (MAP-MRI) and DDE-based axonal modeling were directly compared to reveal the ways in which each approach can specify key features of cellular alterations.
Introduction
Diffusion MRI can reveal nervous system pathology in the absence of other MRI signal changes by its sensitivity to the microscale tissue environment(1-3), although diffusion tensor imaging (DTI)(4) often cannot provide sufficient specificity to detect cellular changes. Several strategies aim to improve this including: 1. Non-Gaussian modeling of water displacement and 2. Double diffusion encoding (DDE) acquisition to probe specific water compartments and geometries. Diffusion Kurtosis Imaging (DKI)(5) and Mean Apparent Propagator MRI (MAP-MRI)(6) are examples of newer strategies to fit multi-shell single-pulsed field gradient DWI data to non-Gaussian signal models that can describe the magnitude and shape of complex environments. DDE strategies can selectively probe restricted water compartments. Axon modeling in coherent white matter (WM) can be used to calculate the average axon diameter (AAD) as well as the axon diameter distribution (ADD) in each voxel(7). Assembling different approaches into a diffusion MRI toolkit could be a powerful way to derive markers of injury, however we must first understand cross-model similarities and differences in the context of microscale pathology. The objective of this study was to perform high-resolution and high-quality DTI, DKI, MAP-MRI and DDE imaging in spinal cord tissue having known pathology and to determine cross-model similarities and differences for detecting key features of axonal injury.Methods
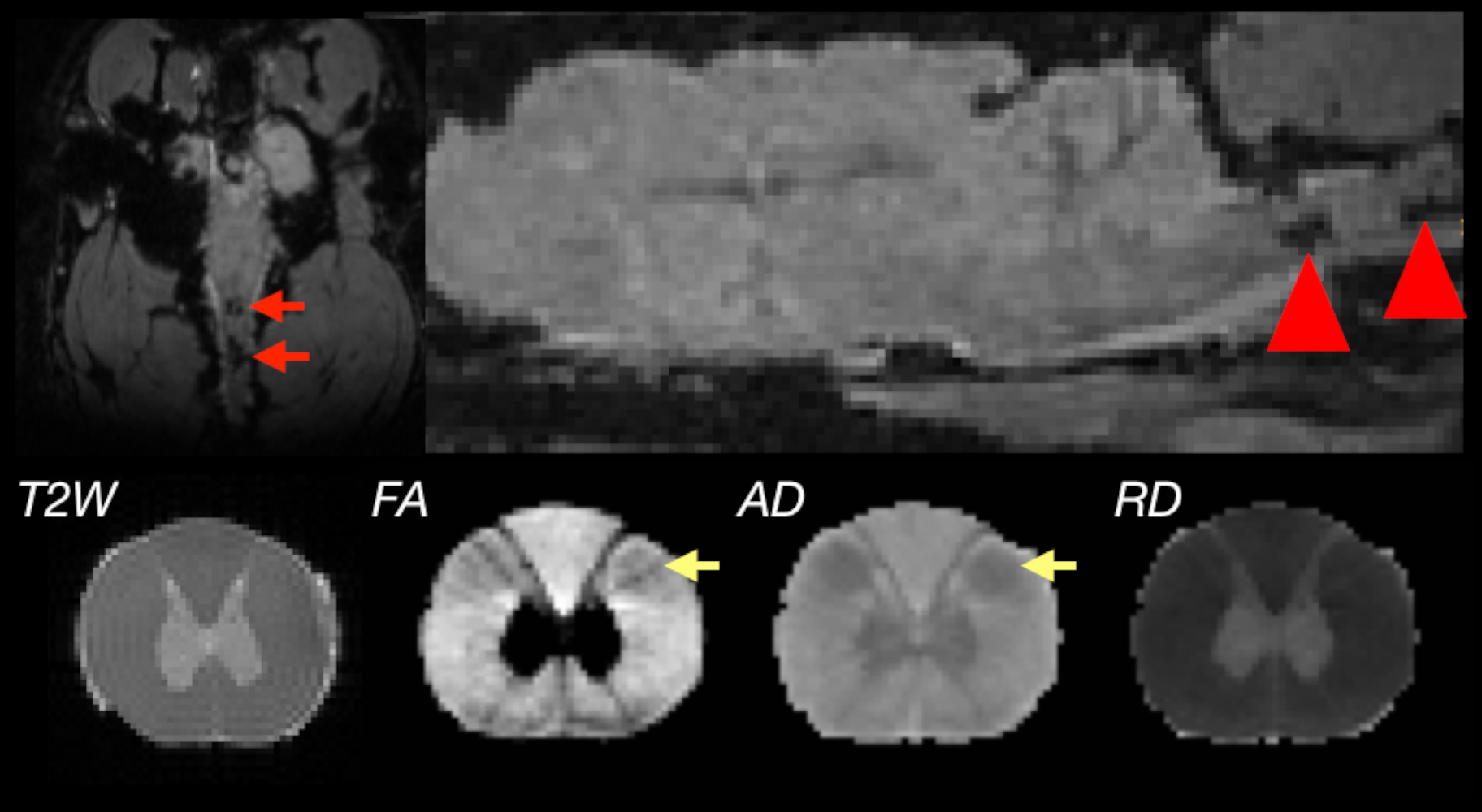
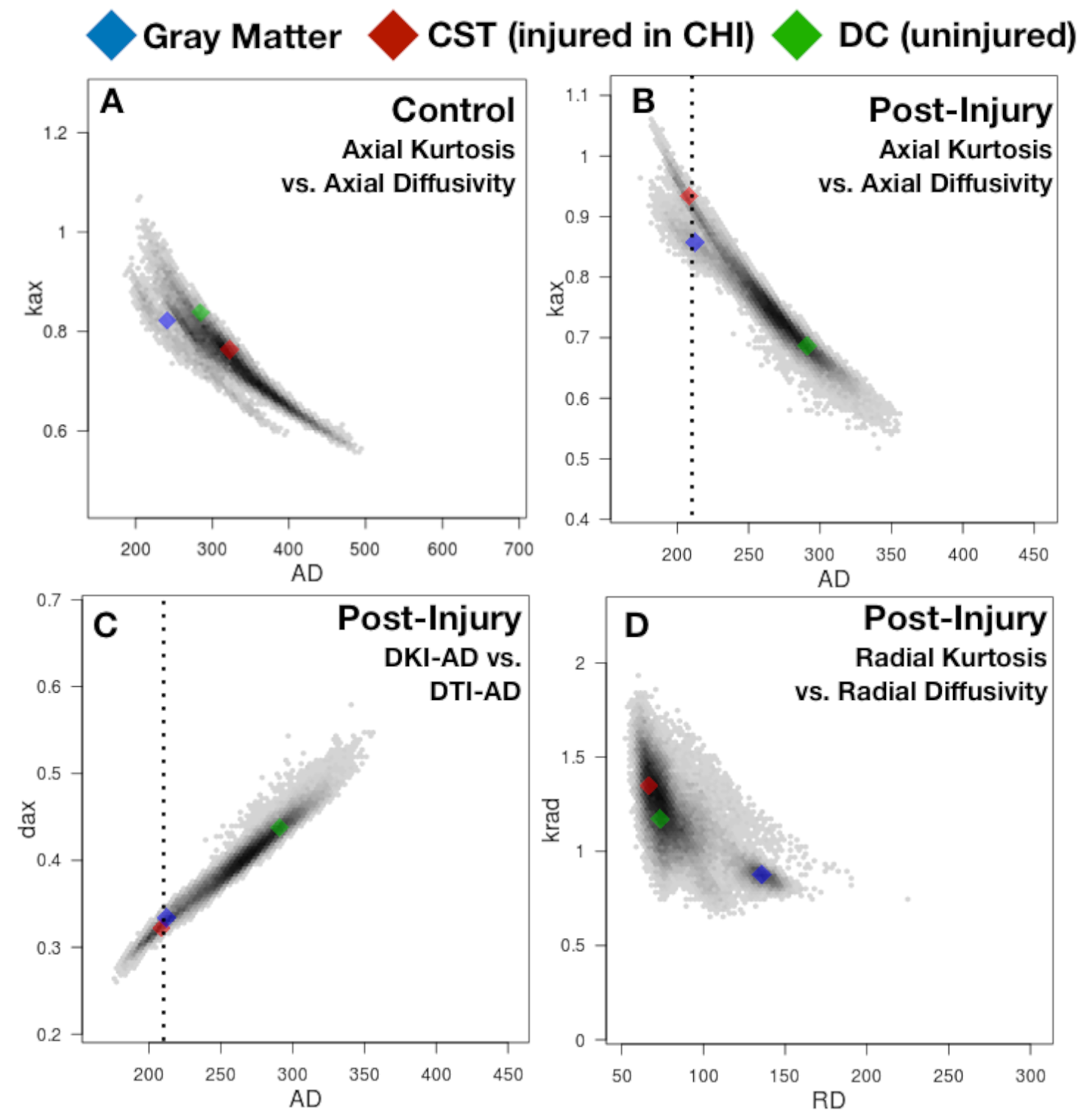
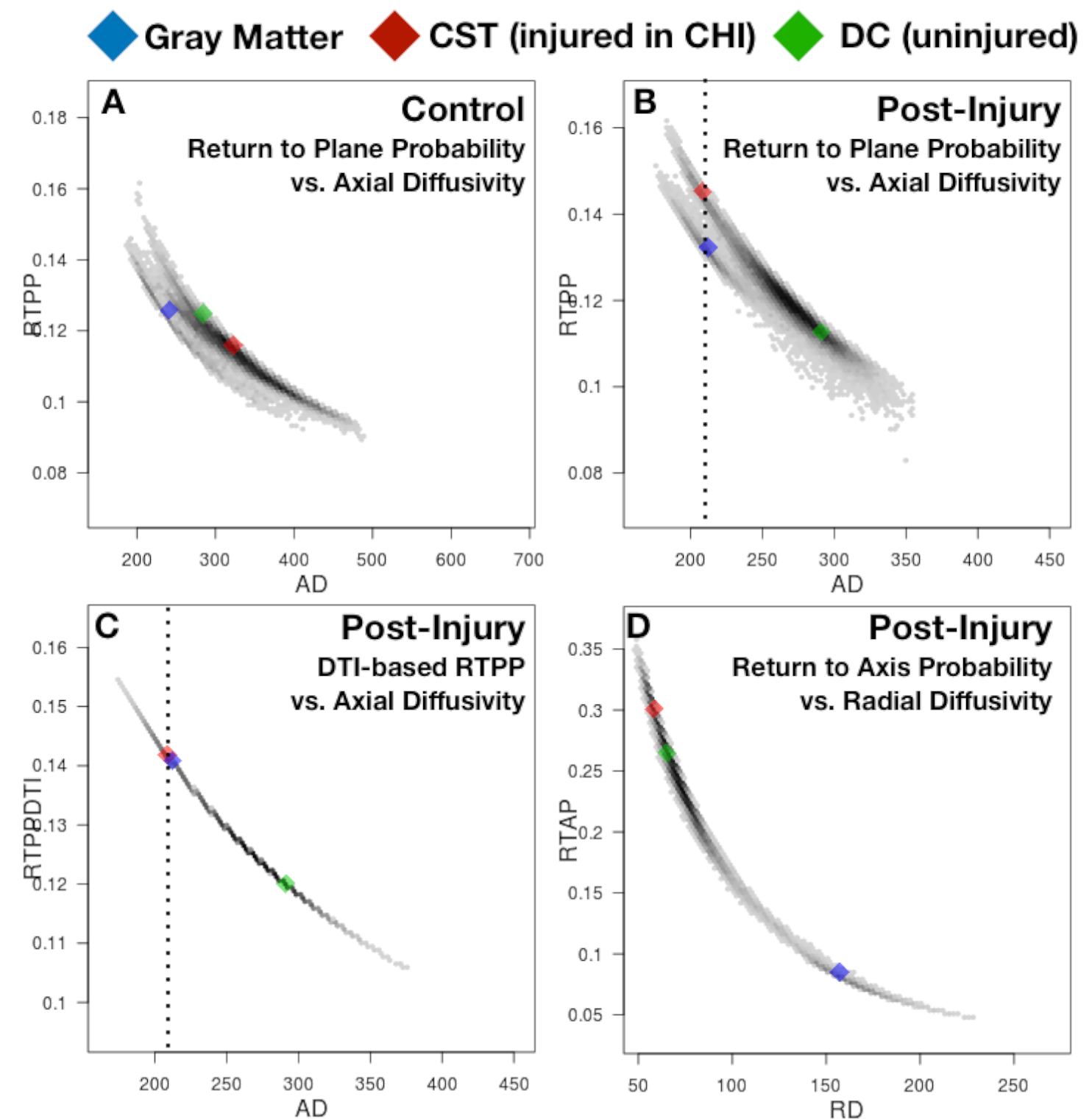
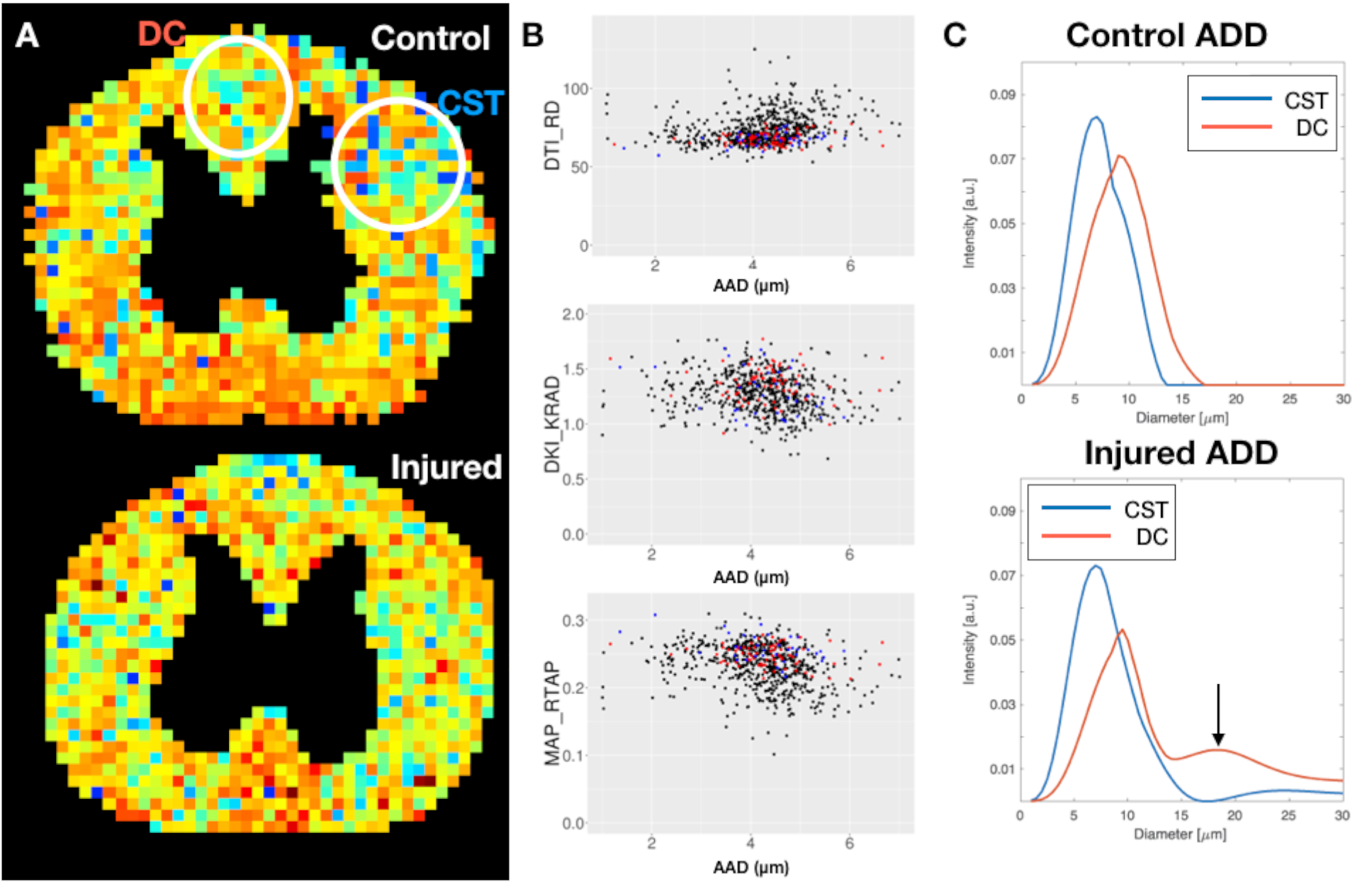
Perfusion fixed spinal cord tissue was obtained from specimens taken as part of a larger study of closed head injury (CHI) in ferrets. Two cervical spinal cord sections were selected, one from an uninjured control and the other 1 week following closed-head injury (CHI) that resulted in focal cortico-spinal tract (CST) hemorrhage (Figure 1A). DWIs were collected using a 5mm linear coil with a 7T Bruker MRI scanner equipped with a microimaging probe using a 3D-EPI pulse sequence. For DTI, DKI and MAP-MRI, 297 DWIs were acquired with b-values from 100-10,000s/mm2; the TORTOISE processing pipeline(8, 9) was used for DWI corrections and for DTI and MAP-MRI fitting. DKI modeling was performed using the diffusion kurtosis estimator(10). For DDE, the following orientation angles were used in the radial plane: 0°:30°:330° g=0-673 mT/m. WM axons were modeled as a pack of impermeable parallel microcapillaries of infinite length with a known orientation. The DDE signal attenuation from the restricted compartment (i.e., axons) was computed using the multiple correlation function (MCF) method(11, 12) and extra-axonal diffusion was modeled as Gaussian(13). 2D histograms showing the correspondence of metric value pairs for all voxels within the imaging volume were generated; average metric value pairs in the CST (injured WM, red), dorsal columns (DC, uninjured WM, green) and ventral horn gray matter (GM, blue) were plotted over the histograms. Metric comparisons were generally made between DTI scalars and their non-Gaussian counterparts; AAD values were compared only with radial diffusivity (RD) obtained from DTI.Results and Discussion
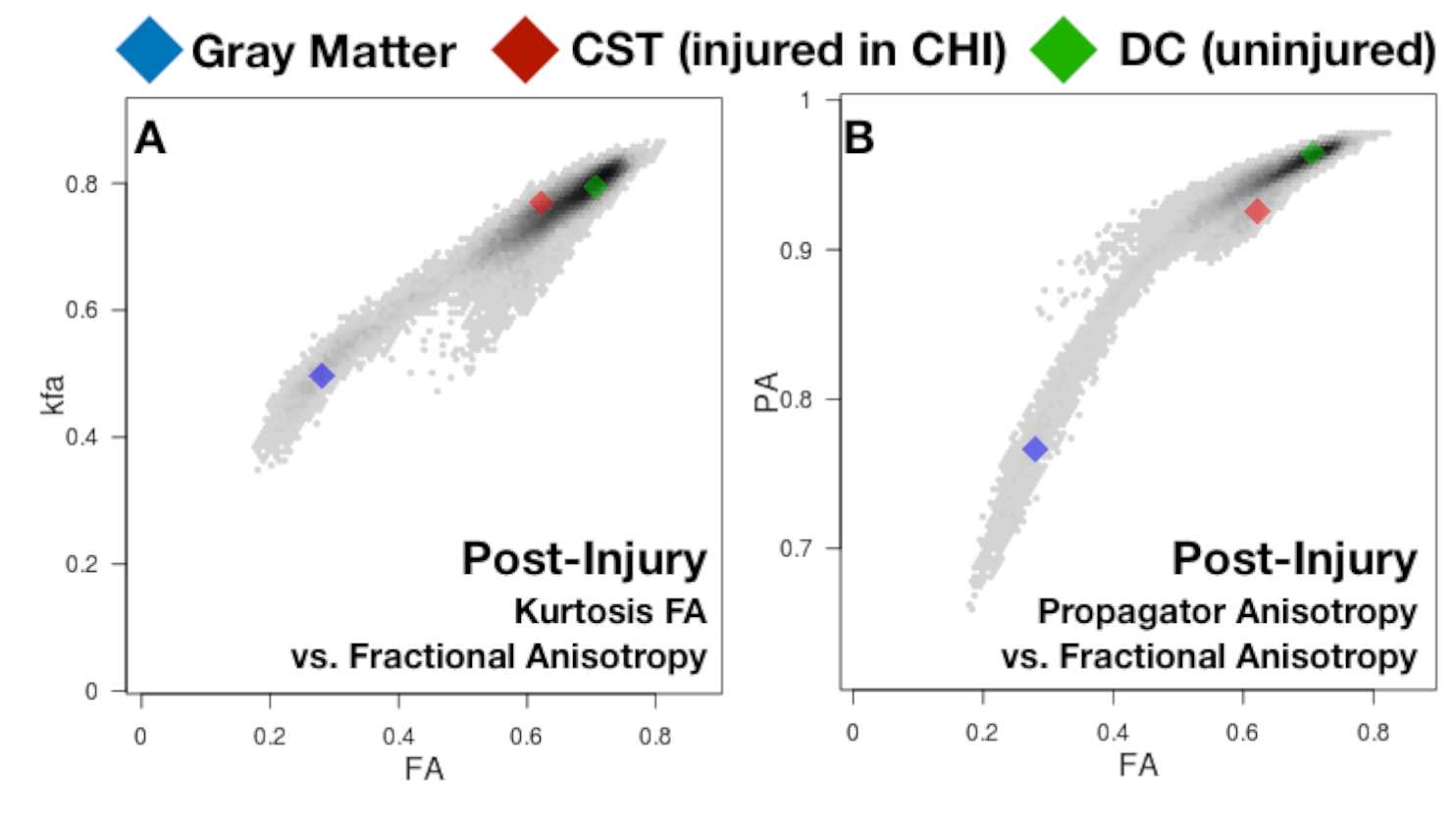
DTI maps from the injured spinal cord (Figure 1) revealed highly localized abnormalities of fractional anisotropy (FA) and axial diffusivity (AD), but not RD and in the absence of T2 weighted image changes. Both axial kurtosis (Kax) and return-to-the-plane probability (RTPP) appeared to distinguish between GM and injured WM having similar AD values, while radial scalars all appeared to have a close relationship (Figures 2 and 3). The distinction of axial information in injured white matter was not observed in DKI-derived AD nor in DTI-based RTPP values, which suggests that this observation is dependent on non-Gaussian signal behavior. Histogram clusters were clearer for MAP-MRI metrics than for DKI metrics; MAP propagator anisotropy (PA) appeared better suited than Kurtosis FA to distinguish injured WM from uninjured WM (Figure 4). This may be related to a better separation of diffusion and kurtosis tensors by full propagator representation by MAP-MRI as opposed DKI. DDE estimates for AAD were not remarkable, but the ADD’s within different ROIs strongly revealed the strength of this approach by showing a second peak in the AAD spectrum or distribution for the injured white matter, but only a single peak in adjacent uninjured WM and in control tissue (Figure 5).Conclusions
Both DKI and MAP-MRI were shown to provide additional information beyond DTI in the axial direction so that injured WM could be quantitatively distinguished from GM. The ability of DDE to reveal a second population of axons with greater diameter in the absence of radial changes suggests potential specificity for detecting beading and demonstrates the ability of this approach to probe changes that may not be accessible to the other techniques.Acknowledgements
This work was supported by the Intramural Research Programs of the National Institute of Biomedical Imaging and Bioengineering and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Ferret spinal cord tissue was obtained as part of a larger study supported by the Center for Neuroscience and Regenerative Medicine (CNRM) administered by the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc.References
1. Budde MD, et al. (2007) Toward accurate diagnosis of white matter pathology using diffusion tensor imaging. Magnetic resonance in medicine 57(4):688-695.
2. Alexander AL, Lee J, Lazar M, & Field AS (2007) Diffusion tensor imaging of the brain. Neurotherapeutics 4(3):316-329.
3. Beaulieu C (2002) The basis of anisotropic water diffusion in the nervous system - a technical review. NMR in Biomedicine 15(7-8):435-455.
4. Basser PJ, Mattiello J, & LeBihan D (1994) MR diffusion tensor spectroscopy and imaging. Biophysical journal 66(1):259-267.
5. Jensen JH, Helpern JA, Ramani A, Lu H, & Kaczynski K (2005) Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magnetic resonance in medicine 53(6):1432-1440.
6. Özarslan E, et al. (2013) Mean apparent propagator (MAP) MRI: a novel diffusion imaging method for mapping tissue microstructure. NeuroImage 78:16-32.
7. Benjamini D, Komlosh ME, Holtzclaw LA, Nevo U, & Basser PJ (2016) White matter microstructure from nonparametric axon diameter distribution mapping. Neuroimage 135:333-344.
8. Irfanoglu MO, Nayak A, Jenkins J, & Pierpaoli C (2017) TORTOISE v3: Improvements and New Features of the NIH Di. 25th Annual Meeting of the International Society for Magnetic Resonance in Medicine.
9. Pierpaoli C, et al. (2010) TORTOISE: an integrated software package for processing of diffusion MRI data. 18th Annual Meeting of the International Society for Magnetic Resonance in Medicine.
10. Tabesh A, Jensen JH, Ardekani BA, & Helpern JA (2011) Estimation of tensors and tensor-derived measures in diffusional kurtosis imaging. Magnetic resonance in medicine 65(3):823-836.
11. Ozarslan E, Shemesh N, & Basser PJ (2009) A general framework to quantify the effect of restricted diffusion on the NMR signal with applications to double pulsed field gradient NMR experiments. The Journal of chemical physics 130(10):104702.
12. Komlosh ME, Benjamini D, & Hutchinson EB (2017) Using double pulsed-field gradient MRI to study tissue microstructure in traumatic brain injury (TBI). Microporous and Mesoporous Materials. 269, 156--159, 2018.
13. Assaf Y & Basser PJ (2005) Composite hindered and restricted model of diffusion (CHARMED) MR imaging of the human brain. Neuroimage. 27; 48-58
Figures