3172
Neuropathologic Correlates of Enlarged Perivascular Spaces in a Community Cohort of Older Adults1Illinois Institute of Technology, Chicago, IL, United States, 2Rush University Medical Center, Chicago, IL, United States
Synopsis
Perivascular spaces are fluid-filled spaces surrounding blood vessels as they penetrate the brain, forming a brain fluid drainage system that facilitates interstitial fluid exchange and clearance of waste products. Enlargement of perivascular spaces is common in aging, and literature has linked enlarged perivascular spaces (EPVS) to increased risk of stroke, lower cognitive function, and vascular dementia. The links of EPVS burden to age-related neuropathologies have not yet been thoroughly investigated. Therefore, the purpose of this work was to assess the neuropathologic correlates of EPVS by combining ex-vivo MRI and pathology data in a large community cohort of 625 older adults.
INTRODUCTION:
Perivascular spaces (PVS), also known as Virchow-Robin spaces, are fluid-filled spaces surrounding blood vessels as they penetrate the brain, forming a brain fluid drainage system that facilitates interstitial fluid exchange and clearance of waste products[1]. Enlargement of perivascular spaces is common in aging, and literature has linked enlarged perivascular spaces (EPVS) to increased risk of stroke[2], lower cognitive function[3], and vascular dementia[4]. In MRI, EPVS appear as hyperintense, and often elongated, features in T2-weighted images[5]. In-vivo MRI studies have associated EPVS burden with aging, hypertension, cerebral amyloid angiopathy, and small-vessel disease[5]-[13]. However, the links of EPVS burden to age-related neuropathologies have not yet been thoroughly investigated. Therefore, the purpose of this work was to assess the neuropathologic correlates of EPVS by combining ex-vivo MRI and pathology data in a large community cohort of older adults.METHODS:
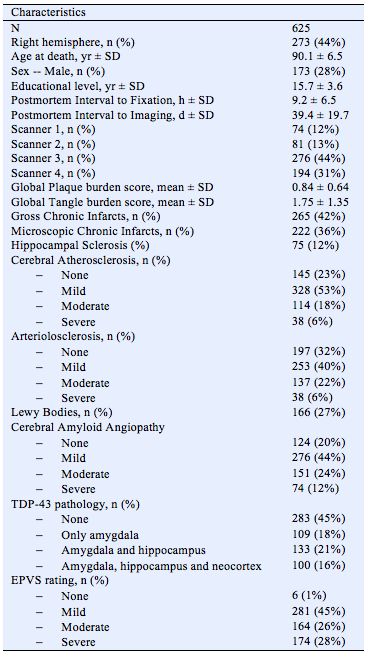
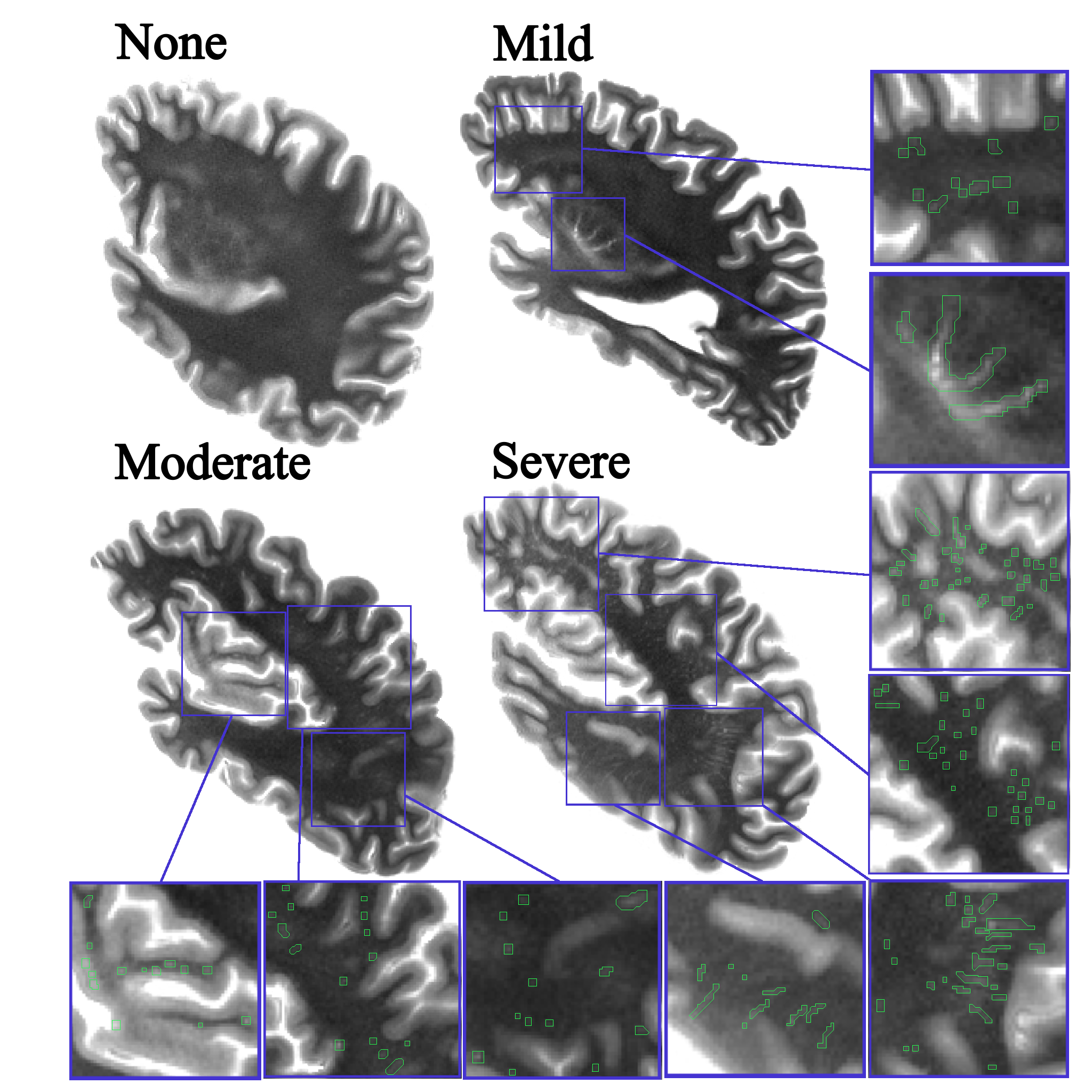
Cerebral hemispheres were obtained from 625 deceased participants of the Rush Memory and Aging Project[14] and Religious Orders Study[15], two longitudinal, epidemiologic clinical-pathologic cohort studies of aging. All hemispheres were imaged on clinical 3T MRI scanners while immersed in 4% formaldehyde solution, with an average postmortem interval to fixation PMIf≈9 hours, and an average postmortem interval to imaging PMIi≈39 days (Fig.1). Following ex-vivo MRI, all hemispheres underwent neuropathologic examination by a board-certified neuropathologist blinded to clinical and imaging findings[16]-[20]. The pathologies assessed included: gross and microscopic infarcts, atherosclerosis, arteriolosclerosis, cerebral amyloid angiopathy, amyloid plaques, neurofibrillary tangles, hippocampal sclerosis, Lewy bodies, and TDP-43. Two experienced observers blinded to all pathologic and clinical data rated EPVS burden in the basal ganglia and white matter throughout the whole brain based on T2-weighted ex-vivo MRI data, using a semiquantitative four-level scale (none=0, mild=1, moderate=2, severe=3) (Fig.2). Intra-rater and inter-rater reliability were assessed using the intraclass correlation (ICC). Statistical analysis involved a two-step process, including univariate logistic regression where EPVS burden was the dependent variable and each pathology was the independent variable, followed by multivariate logistic regression where EPVS burden was the dependent variable and all pathologies where considered in the same model as independent variables, also controlling for age, sex, education, PMIf, PMIi, and scanners.
RESULTS:
Participants’ age at the time of death was [65.9-108.3 years] with a mean of 90.1±6.5 years, and 28% of the participants were male (Fig.1). Both intra-rater (ICC=0.88) and inter-rater reliability (ICC=0.75) for EPVS rating were good[21]. The distribution of EPVS scores of 0 to 3 among participants of this community cohort was 6 (1%), 281 (45%), 164 (26%) and 174 (28%) participants, respectively. Due to the small number of participants with a score of 0, scores of 0 and 1 were merged into one level. Univariate analyses showed significant association of EPVS burden with gross infarcts (OR=1.66, p-value<0.001) and TDP-43 pathology (OR=0.86, p-value=0.024). Multivariate logistic regression considering all pathologies and covariates showed a significant association of EPVS burden with gross infarcts (OR=1.67, p=0.002).
DISCUSSION:
The present work demonstrated that EPVS burden is associated with gross infarcts in a community cohort of older adults. This suggests that the two abnormalities may share similar neurobiological pathways. It has been suggested that stiffening of the arterioles in small-vessel disease impairs interstitial fluid drainage along PVS and causes EPVS, and that ischemia might occur secondary to endothelial dysfunction and impaired autoregulation in stiffened vessels unable to respond to vasodilatory stimuli during exertion[22].
The
work presented here is the largest investigation on the neuropathologic
correlates of EPVS in a community cohort. Other strengths of this work include the
combination of MRI with histopathology which provides the gold standard when
studying age-related neuropathologies, the comprehensive list of
neuropathologies investigated, and the use of ex-vivo MRI which eliminates the
possibility of additional pathology developing in the time interval between
imaging and autopsy.
CONCLUSION:
The present study provides robust evidence on the neuropathologic correlates of EPVS in a large community cohort of older adults. The results suggest that EPVS and gross infarcts may share similar neurobiological pathways, which is in agreement with the literature on the etiologies driving these two processes.Acknowledgements
UH2-UH3 NS100599References
[1] – Brown R., et al. "Understanding the role of the perivascular space in cerebral small vessel disease." Cardiovascular research 114.11 (2018): 1462-1473.
[2] - Selvarajah J., et al. "Potential surrogate markers of cerebral microvascular angiopathy in asymptomatic subjects at risk of stroke." European radiology 19.4 (2009): 1011-1018.
[3] - MacLullich A.M.J., et al. "Enlarged perivascular spaces are associated with cognitive function in healthy elderly men." Journal of Neurology, Neurosurgery & Psychiatry 75.11 (2004): 1519-1523.
[4] - Patankar T.F., et al. "Dilatation of the Virchow-Robin space is a sensitive indicator of cerebral microvascular disease: study in elderly patients with dementia." American Journal of Neuroradiology 26.6 (2005): 1512-1520.
[5] – Wardlaw J.M., et al. "Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration." The Lancet Neurology 12.8 (2013): 822-838.
[6] – Hurford R., et al. "MRI-visible perivascular spaces: relationship to cognition and small vessel disease MRI markers in ischaemic stroke and TIA." J Neurol Neurosurg Psychiatry 85.5 (2014): 522-525.
[7] – Potter G.M., et al. "Enlarged perivascular spaces and cerebral small vessel disease." International journal of stroke 10.3 (2015): 376-381.
[8] – Zhu Y.C., et al. "Severity of dilated Virchow-Robin spaces is associated with age, blood pressure, and MRI markers of small vessel disease: a population-based study." Stroke 41.11 (2010): 2483-2490.
[9] – Rouhl R.P.W., et al. "Virchow-Robin spaces relate to cerebral small vessel disease severity." Journal of neurology 255.5 (2008): 692-696.
[10] - Gutierrez J., et al. "Brain Perivascular spaces as biomarkers of vascular risk: results from the northern Manhattan study." American Journal of Neuroradiology (2017).
[11] - Doubal F.N., et al. "Enlarged perivascular spaces on MRI are a feature of cerebral small vessel disease." Stroke 41.3 (2010): 450-454.
[12] - Martinez-Ramirez S., et al. "Perivascular Spaces Volume in Sporadic and Hereditary (Dutch-Type) Cerebral Amyloid Angiopathy." Stroke 49.8 (2018): 1913-1919.
[13] - Charidimou A., et al. "White matter perivascular spaces An MRI marker in pathology-proven cerebral amyloid angiopathy?." Neurology 82.1 (2014): 57-62.
[14] – Bennett D.A., et al. "Overview and findings from the Rush Memory and Aging Project." Current Alzheimer Research 9.6 (2012): 646-663.
[15] – Bennett D.A., et al. "Overview and findings from the Religious Orders Study." Current Alzheimer Research 9.6 (2012): 628-645.
[16] – Schneider J.A., et al. "Cognitive impairment, decline and fluctuations in older community-dwelling subjects with Lewy bodies." Brain 135.10 (2012): 3005-3014.
[17] - Dawe R.J., et al. "Ex vivo T2 relaxation: associations with age-related neuropathology and cognition." Neurobiology of aging 35.7 (2014): 1549-1561.
[18] - Schneider J.A., et al. "Cerebral infarctions and the likelihood of dementia from Alzheimer disease pathology." Neurology 62.7 (2004): 1148-1155.
[19] - Schneider J.A., et al. "Cognitive impairment, decline and fluctuations in older community-dwelling subjects with Lewy bodies." Brain 135.10 (2012): 3005-3014.
[20] - Arvanitakis Z., et al. "Microinfarct pathology, dementia, and cognitive systems." Stroke 42.3 (2011): 722-727.
[21] – Koo T.K., et al. “A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research.” J Chiropr Med 15 (2016: 155-163.
[22] - Wardlaw J.M., et al. "Mechanisms of sporadic cerebral small vessel disease: insights from neuroimaging." The Lancet Neurology 12.5 (2013): 483-497.
Figures