3171
Quantitative Intracranial Vasculature Assessment to detect dementia using the intraCranial Artery Feature Extraction (iCafe) Technique1University of Washington, Seattle, WA, United States, 2Kaiser Permanente Washington Health Research Institute, Seattle, WA, United States
Synopsis
Intracranial artery features measured from 3D magnetic resonance angiography (MRA) may provide new biomarkers for detecting dementia. Quantitative morphometry and intensity features using iCafe analysis of MRA was compared between cognitively normal and abnormal subjects. We found significantly lower total artery length (p=0.0046), distal artery length (p=0.0043), number of branches (p=0.0038) and average order (p=0.0250) in the cognitively abnormal group. These results suggest reduced vascularity for dementia subjects. iCafe is a promising tool to quantitatively characterize intracranial vascular structures for dementia research.
INTRODUCTION
Dementia is a common disease of the elderly that not only affects quality of life but also reduces lifespan. Despite intensive research in this field, there are no reliable methods to identify subjects at risk for dementia. Vascular factors such as diabetes, hypertension and atherosclerosis are known to increase the odds of dementia1–3. Thus assessment of the intracranial vasculature may provide new biomarkers for detecting dementia risk. MR angiography (MRA) although clinically used for detecting vascular pathologies, has not been used as a comprehensive vascular assessment tool due to the complexity of information available in MRA.
Recently, the intraCranial artery feature extraction (iCafe)4 technique has been demonstrated to provide quantitative morphometry and intensity features for vasculature visible from 3D time-of-flight (TOF) MRA. Decrease in intracranial blood flow is reflected as decreased length and higher order branch measurements. We hypothesize that distal artery measurements by iCafe reflecting blood flow decrease that is known to occur with dementia5 can be used to distinguish normal vs abnormal cognitive status. The Adult Changes in Thought study (ACT) is a prospective longitudinal study of cognitive health of a community-based cohort6 where the participants are followed up with cognitive assessment every two years until diagnosis of dementia and/or Alzheimer's disease. Thus the ACT cohort is well characterized in terms of cognitive ability.
Aim: To identify whether iCafe vascular biomarkers differ between a group of dementia and healthy subjects in participants of the ACT Study.
METHODS
Patient studies
Forty-one subjects (age 78.3±5.7 years, 19 males) were recruited from the ACT cohort. Based on their cognitive assessments, subjects were divided into healthy and dementia groups. Twenty-six subjects were cognitive normal, and the dementia group included seven subjects with minor cognitive impairment (MCI), two subjects with Alzheimer's disease (AD), and six with other dementia types (OD).
MR imaging
After informed consent 3D TOF images were scanned on a 3.0T Philips (Best, The Netherlands) Achieva MR scanner under local IRB guidelines. A 32-channel head coil (Philips Healthcare, Best, The Netherlands) was used. 3D TOF parameters were as follows: TR/TE = 14/3.5 ms, flip angle = 18°, in-plane resolution = 0.30 mm×0.30 mm, slice thickness = 1.4 mm, field of view = 190 mm*190 mm.
Feature extraction
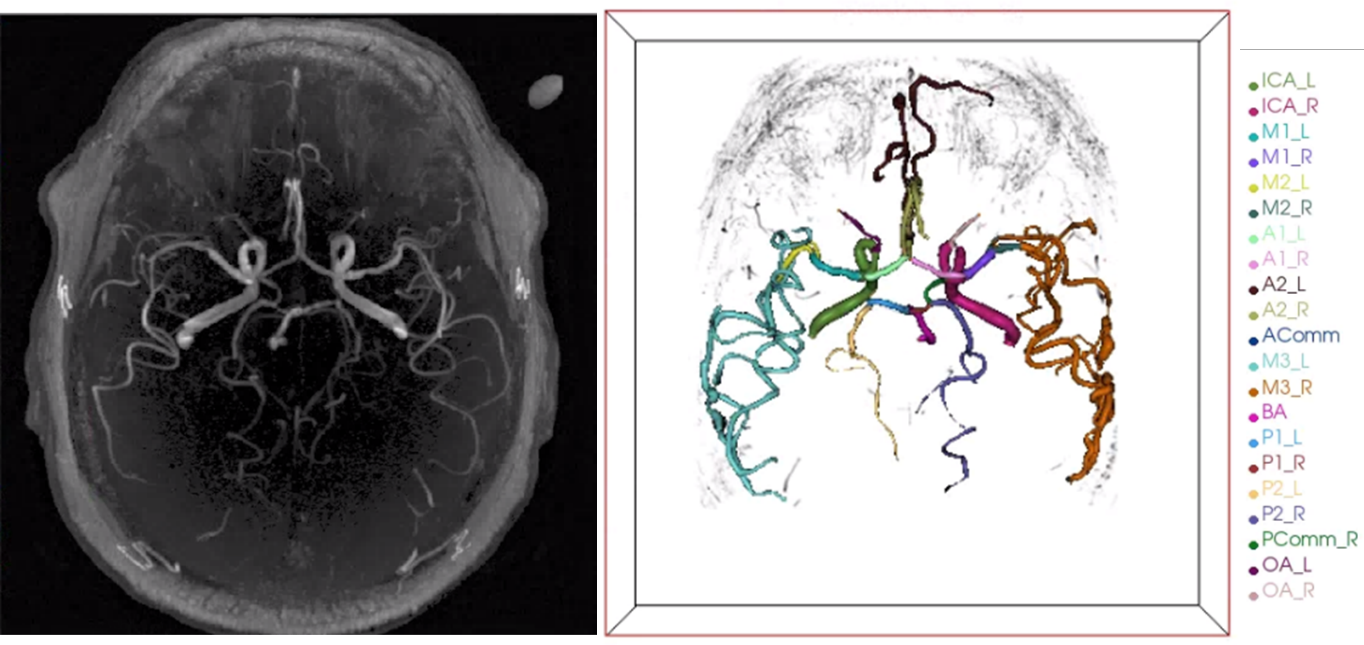
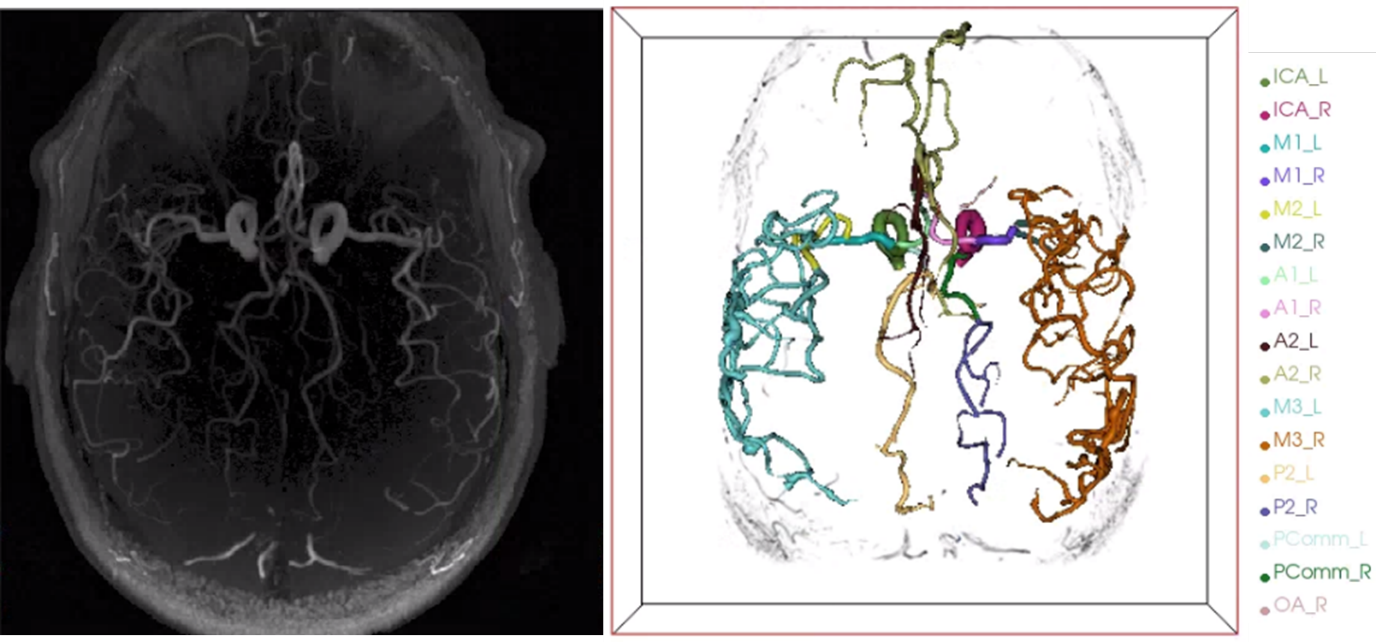
TOF images were resampled to isotropic resolution of 0.30 mm and image intensities were normalized using the Nyul7 method to allow comparable intensity features from different cases in dataset. Artery regions were then traced using an improved open-curve active contour model, and labeled using a maximum a posteriori model in iCafe. An experienced iCafe operator blinded to cognitive assessment, supervised the tracing and labeling process and made corrections when needed. Artery traces from one subject with AD and one healthy subject are shown in Figure 1 and Figure 2, respectively.
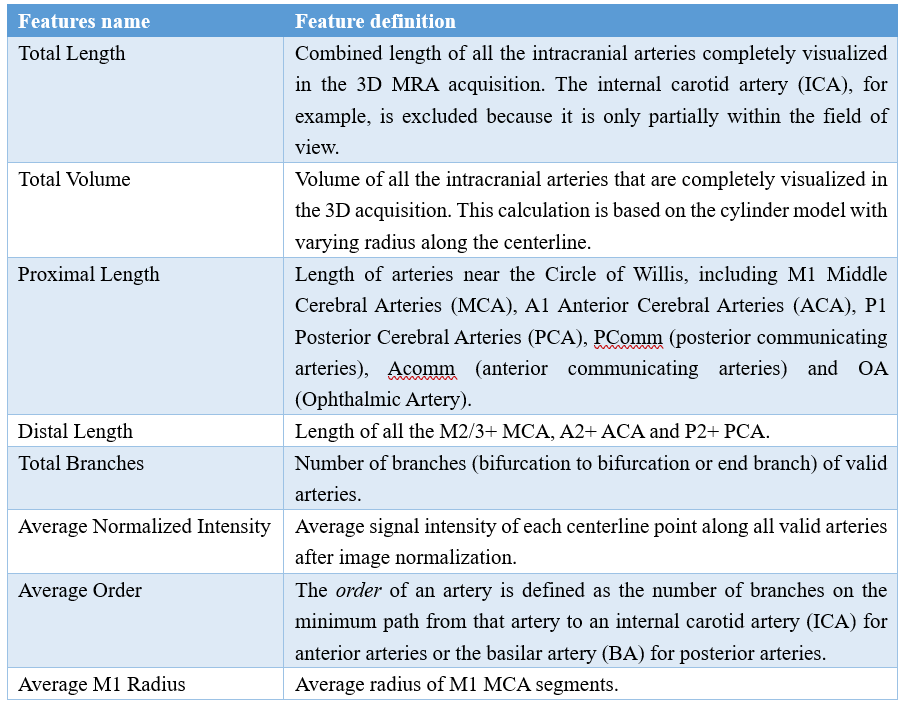
A group of representative features (listed in Table 1) reflecting typical intracranial arterial characteristics were quantified using iCafe.
Statistical Testing
Student’s t test was used to assess the difference for healthy and dementia groups of each feature. P<0.05 was considered as statistically significant without adjustment for the number of comparisons.
RESULTS
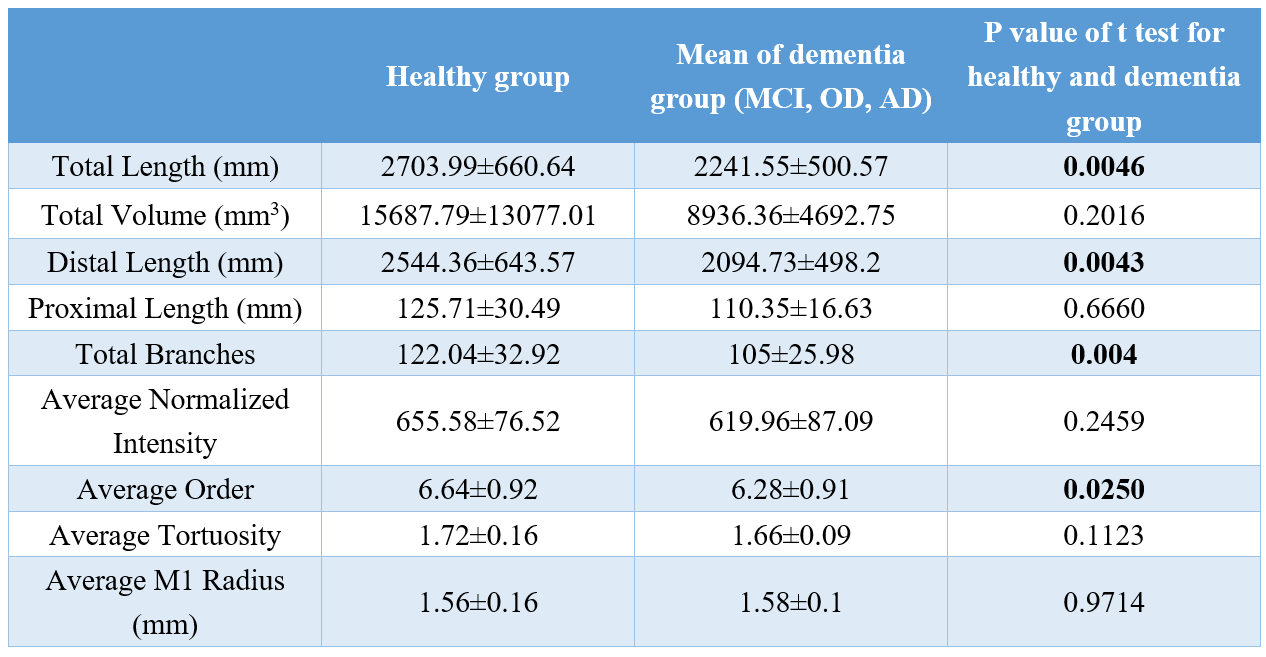
Representative features extracted from iCafe for healthy and dementia groups are shown in Table 2. The dementia group had significantly lower total artery length (p=0.0046). Further dividing the arteries into proximal and distal subgroups, the dementia group had significantly lower distal length (p=0.0043), but not proximal length (p=0.6660). The dementia group also had a lower number of branches (p=0.0038) and average branch order (p=0.0250). Other vascular features did not show significant differences.DISCUSSION
iCafe measurements were able to distinguish between normal and cognitively impaired groups. We found relatively reduced vasculature for dementia group. This is likely due to reduced blood flow with dementia and therefore reduced visibility of the more distal intracranial arteries on TOF MRA. Since visibility of distal vessels on TOF are first reduced with decreased flow, the reduction in distal vessel length and not proximal vessel length suggests that blood flow decrease may be an indicator for reduced cognitive function.
Although only forty-one subjects were used, iCafe measurements were able to distinguish between the two groups suggesting that iCafe quantification of MRA may provide high sensitivity to detect subjects with dementia.
CONCLUSION
Using a semi-automated quantitative analysis tool (iCafe), differences in intracranial arterial features were identified on TOF-MRA between cognitively normal individuals and those with mild cognitive impairment or dementia. Distal artery length measurement by iCafe is reduced in subjects with MCI or dementia compared to cognitively normal subjects. The quantitative information provided by iCafe is promising for a comprehensive description of intracranial artery status in dementia.Acknowledgements
This research is supported by grants from National Institute of Health (U01AG006781, R01-NS092207, R01-HL103609) and Philips Healthcare.References
1. Breteler MMB. Vascular involvement in cognitive decline and dementia. Epidemiologic evidence from the Rotterdam study and the Rotterdam scan study. In: Annals of the New York Academy of Sciences. Vol 903. Wiley/Blackwell (10.1111); 2000:457-465. doi:10.1111/j.1749-6632.2000.tb06399.x.
2. Fontbonne A, Berr C, Ducimetiere P, Alperovitch A. Changes in cognitive abilities over a 4-year period are unfavorably affected in elderly diabetic subjects: Results of the epidemiology of vascular aging study. Diabetes Care. 2001;24(2):366-370. doi:10.2337/diacare.24.2.366.
3. Knopman D, Boland LL, Mosley T, et al. Cardiovascular risk factors and cognitive decline in middle-aged adults. Neurology. 2001;56(1):42-48. doi:10.1212/WNL.56.1.42.
4. Chen L, Mossa-Basha M, Balu N, et al. Development of a quantitative intracranial vascular features extraction tool on 3D MRA using semiautomated open-curve active contour vessel tracing. Magn Reson Med. 2018;79(6):3229-3238. doi:10.1002/mrm.26961.
5. Kukull WA, Higdon R, Bowen JD, et al. Dementia and Alzheimer Disease Incidence. Arch Neurol. 2002;59(11):1737. doi:10.1001/archneur.59.11.1737.
6. J. Montine T, A. Sonnen J, S. Montine K, K. Crane P, B. Larson E. Adult Changes in Thought Study: Dementia is an Individually Varying Convergent Syndrome with Prevalent Clinically Silent Diseases that may be Modified by Some Commonly Used Therapeutics. Curr Alzheimer Res. 2012;9(6):718-723. doi:10.2174/156720512801322555.
7. Nyul LG, Udupa JK, Zhang X. New variants of a method of MRI scale standardization. IEEE Trans Med Imaging. 2000;19(2):143-150. doi:10.1109/42.836373.
Figures