3164
Vascular disease risk factors in multiple sclerosis is associated with reduced cerebral metabolic activity1Advanced Imaging Research Center, Oregon Health & Science University, Portland, OR, United States, 2Department of Neurology, Oregon Health & Science University, Portland, OR, United States, 3VA Portland Health Care System, Portland, OR, United States
Synopsis
Reduced cerebral metabolic activity is observed with increased vascular disease risk factors like hyperlipidemia, hypertension, obesity, diabetes, and heart disease. High resolution MR techniques are used to measure and characterize capillary water flux and water permeability surface product as potential surrogates of brain metabolic activity.
Purpose:
Investigate effect of vascular disease factors on brain tissue metabolism using capillary water flux measurements by a high resolution MRI metabolic mapping technique at 7T.Introduction:
Decreased cerebral metabolism resulting from vascular disease risk factors could substantially increase the risk of neurodegeneration in MS.1,2 Capillary water flux can be measured using high-resolution MR techniques3 and is driven by local metabolic activity through endothelial membrane proteins such as Na+/K+- ATPase.4 Therefore, the capillary water flux and water permeability surface product (P Methods:S) are potential surrogates of brain metabolic activity. The goal of this study was to assess capillary water flux in individuals with multiple sclerosis (MS) with and without vascular disease risk factors, VDRF+, VDRF-, respectively
Methods:
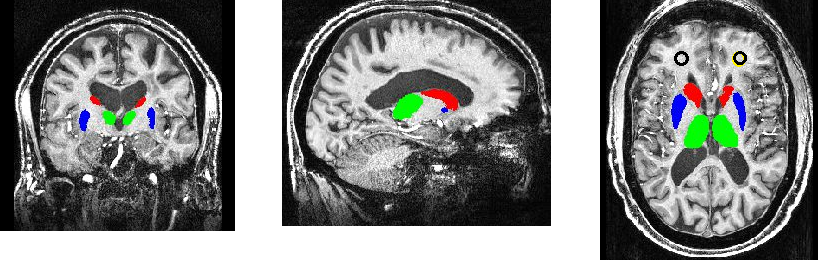
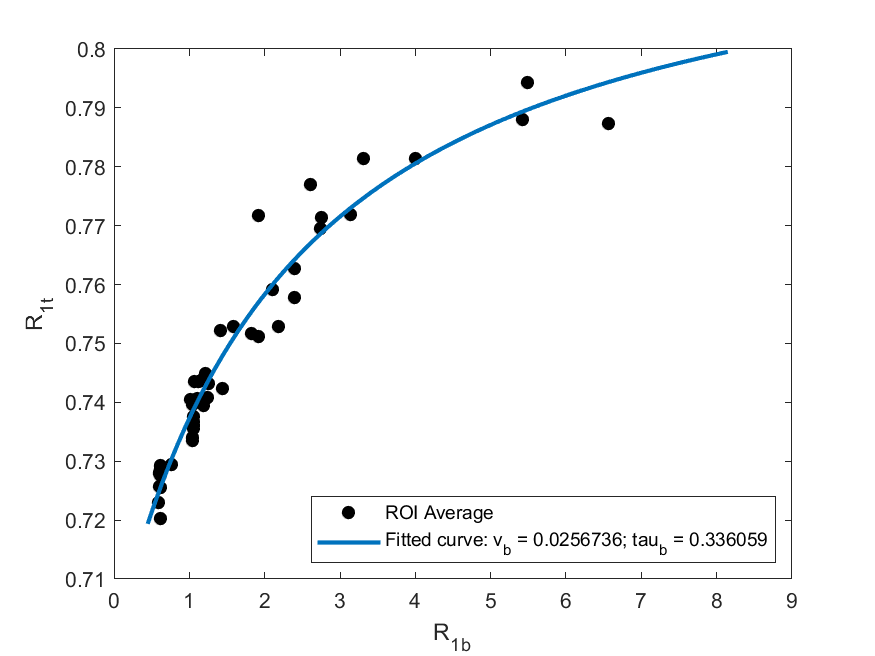
Fifty MS subjects underwent dynamic contrast enhanced imaging with a 7T MRI instrument (Siemens Healthineers). Individuals with MS were divided into two groups; VDRF+, and VDRF-. The VDRF+ group included individuals with one or more of the following conditions hyperlipidemia, hypertension, obesity, diabetes, and heart disease. A T1-weighted 3D-spoiled gradient echo sequence with whole-brain coverage (TR/TE/FA: 2.7ms/1.2ms/6°, 44 axial slices, 5 mm slice thickness, 3.6 s temporal resolution, 80 volumes) was obtained. Two gadoteridol (ProHance; Bracco, Cranberry, NJ) administrations, the first with 0.0143 mmol/kg, and the second (8 minutes after the first) with a 0.0286 mmol/kg dose each were injected at 2 mL/s and followed by a 20 mL saline flush. R1 maps were calculated on a voxel-wise basis. The bilateral thalami were segmented with FLIRT using bias-corrected T1-w MPRAGE scans as an input (Figure 1).4 Mean blood volume fraction (vb) and equilibrium water extravasation rate constant (kpo) values within the thalami were determined by non-linear modeling with the following equation3 using MATLAB (MathWorks, Inc., Natick, MA) (Figure 2):
R1t(t) = (1/2){ [R1b(t) + R1e + kpo + kpo pb/(1-pb)] - [(R1e - R1b(t) - kpo + kpo pb/(1-pb))2 + 2(kpo)2 pb/(1-pb)]1/2}
where pb is the mole fraction of tissue water in blood (vb=pb·fw, fw is the tissue volume fraction accessible to mobile aqueous solutes), R1t(t) is the tissue R1, R1b(t) is the R1 of blood, time-dependent due to differential plasma concentration of gadoteridol, and was measured from the R1 map in the sagittal sinus. PwS was calculated as the product of vb and kpo.
Results:
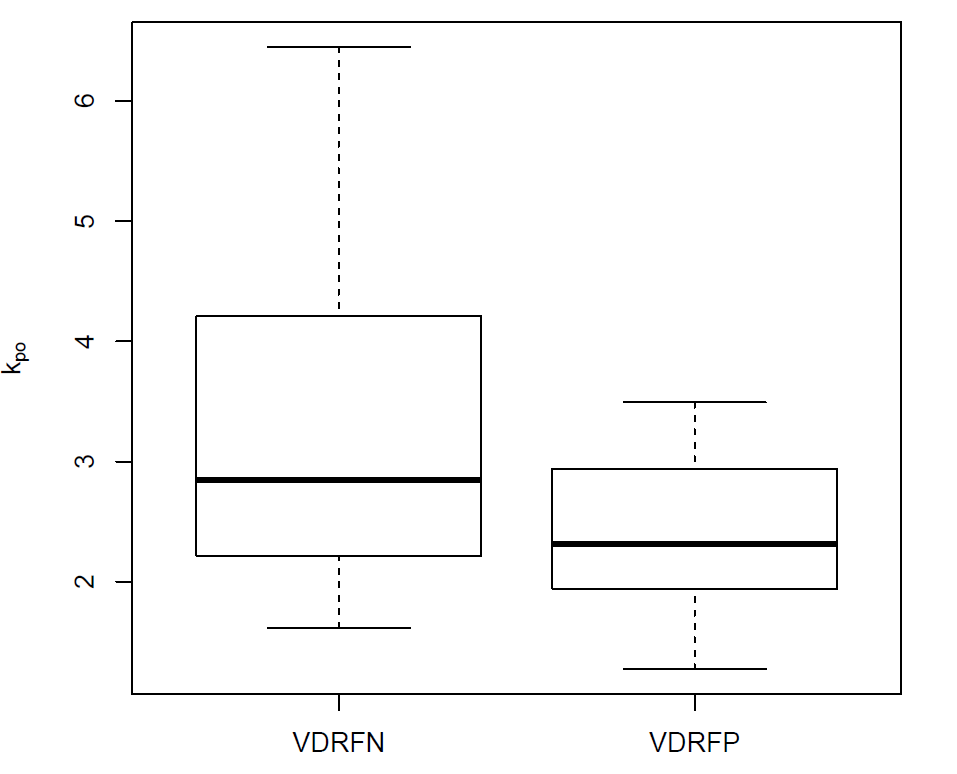
The VDRF+ group was comprised of 28 individuals (mean age 56.4 years (SD: 6.9), 82% female), and the VDRF- group was comprised of 22 individuals (mean age 52.2 years (SD: 7.8); 59% female). Average thalami kpo was significantly lower in the VDRF+ group compared to compared to VDRF- group (mean ± SD: VDRF+ 2.45 ± 0.65 s-1; VDRF- 3.45 ± 1.31 s-1; p= 0.007). The water permeability surface area product (PWS = kpo*vb), a putative measure of tissue average metabolic activity was reduced in VDRF+ compared to VDRF- (VDRF+ 0.083 ± 0.025 s-1; VDRF- 0.071 ± 0.016 s-1; p = 0.024). The blood volumes, vb, were not significantly different between groups (VDRF+ 0.030 ± 0.007; and VDRF- 0.027 ± 0.007; p = 0.14).Discussion:
Reduced PwS in thalami suggests decreased metabolic activity in MS individuals with VDRF+ compared to VDRF-. There was no significant difference in vb and reduced kpo was the primary driver for reduced PwS; kpo is the average capillary water flux rate constant. The approach described here has the potential to provide high-resolution metabolic activity maps which could be used to identify tissue at risk for neurodegeneration and also serve as a biomarker for therapeutic interventions. PwS and other DCE-derived parameters are promising as potential biomarkers, however, further studies needed to validate their use.Acknowledgements
Funding: VA Merit 1I01RX001636-01A1; Conrad N Hilton Innovation Fund; NIH OD018224; NMSS FG-16-7-25259
References
- Lassmann H, van Horssen J, Mahad D. Progressive multiple sclerosis: pathology and pathogenesis. Nature reviews Neurology. 2012;8(11):647-656.
- Mahad DH, Trapp BD, Lassmann H. Pathological mechanisms in progressive multiple sclerosis. The Lancet Neurology. 2015;14(2):183-193.
- Rooney WD, Li X, Sammi MK, et al. Mapping human brain capillary water lifetime: high-resolution metabolic neuroimaging. NMR in biomedicine. 2015;28(6):607-623.
- Fischl B, Salat DH, Busa E, et al. Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron. 2002;33(3):341-355.
Figures