3163
Investigating the contribution of interhemispheric disconnection to disability and fatigue in Progressive Multiple Sclerosis.1Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2University of Verona, Verona, Italy, 3University of Genoa/IRCCS AOU San Martino-IST, Genova, Italy
Synopsis
We explored the presence and clinical impact of interhemispheric disconnection in progressive multiple sclerosis (PMS) through a tractography-based approach, quantifying the number of streamlines passing through callosal subregions. In PMS, we identified a reduced number of streamlines in the splenium and the anterior portion of the corpus callosum (CC) body. Patients with primary and secondary progressive phenotype presented different patterns of CC involvement. The reduced number of streamlines in central and anterior CC was related to motor disability and fatigue, while loss of the integrity in the posterior portion of CC was the main feature of cognitively impaired patients.
Purpose
Callosal damage and disconnection have been described across different multiple sclerosis (MS) phenotypes, in relationship with both motor and cognitive disability. Motor callosal disconnection has been reported at the earliest stages of relapsing-remitting MS (RRMS), prior to development of macroscopic lesion and in presence of preserved motor function1. In benign MS, deficit of executive functions and verbal learning are associated with decreased mean fractional anisotropy (FA) in the body and genu of the corpus callosum (CC)2. Moreover, in primary-progressive MS (PPMS) baseline callosal damage, quantified with a voxel-wise analysis of FA, is able to predict motor and cognitive disability progression at 5-year follow-up3. Based on this background, we decided to investigate the integrity of callosal subregions in a group of primary and secondary progressive MS patients (PMS) through a tractography-based approach, and to explore the clinical impact of interhemispheric disconnection on objective disability and perceived fatigue.Methods
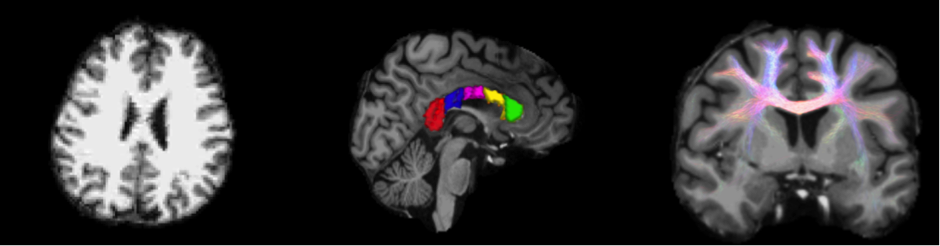
Twenty-four PMS patients (16F, mean age 54.8±9.3 years; 12 PPMS, 6F, mean age 53.0±10.9 years and 12 SPMS, 10F, mean age 57.0±6.7years) and 18 healthy controls (HC) (8F, mean age 50.4±7.9 years) were prospectively enrolled. Patients were classified as cognitively impaired (CI) when showing z-scores ≤ -2 in at least 2 cognitive domains of the minimal assessment of cognitive function in MS (MACFIMS) battery. All subjects underwent MRI on a Siemens Skyra 3T. The protocol included: 3D T2-weighted image and T1-weighted magnetization-prepared rapid gradient echo (MPRAGE) image with voxel size 1x1x1mm3, and a DKI sequence with b-values of 1000, 2000s/mm2 and 30 directions each in addition to b=0s/mm2 images and voxel size of 2×2×2mm3. For the PMS patients white matter lesions were outlined on T2-W and T1-W images and a lesion filling was applied on T1-W images to perform tractography with ACT4. DKI images were corrected for motion and eddy currents and used to perform tractography with iFOD2 algorithm5 implemented in MRtrix3. From the global tractography obtained, the streamlines passing through the CC were extracted using the FreeSurfer classical parcellation in 5 portions: anterior, mid-anterior, central, mid-posterior and posterior (Figure 1). The number of streamlines passing through these portions was used to perform between-groups ANOVA and to test partial correlations with the Expanded Disability Status Scale (EDSS) and the Modified Fatigue Impact Scale (MFIS). Age and gender were entered as covariates in all statistical analysis, as well as the volume of the considered CC portion in each subject, in order to account for anatomical variability. Correlations were further adjusted for disease duration.Results and Discussion
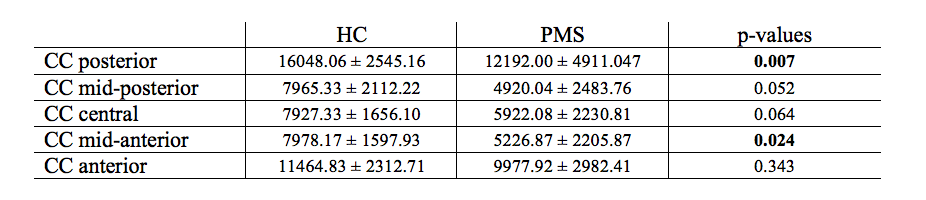
When compared with HC, PMS patients showed a significantly lower number of streamlines passing through posterior (p=0.007) and mid-anterior (p=0.024) CC. Differences in the other CC portions, although present, did not reach the statistical threshold. The results of the between group comparison (PMS vs HC) are summarized in Table 1. A post-hoc analysis conducted on the patient subgroups showed: (i) significant differences between SPMS and HC in posterior (p=0.027), central (p=0.008) and mid-anterior (p=0.006) CC, and between PPMS and HC in posterior CC (p=0.018); (ii) significant differences between CI patients and HC in posterior (p=0.007) and mid-anterior (p=0.05) CC. Global motor disability, expressed by EDSS, was negatively correlated with the number of streamlines passing through central and anterior CC. Likewise, global fatigue was correlated with the number of streamlines passing through central CC and showed a correlation trend with anterior CC. While disconnection in central CC was related to physical fatigue, disconnection in anterior CC was related to both physical and psychosocial fatigue. Two-tails partial correlation results with the clinical scores are summarized in Table 2.Conclusion
The analysis of CC integrity confirms the presence of an interhemispheric disconnection in PMS, mainly affecting the splenium and the anterior portion of the CC body. PPMS and SPMS patients presented different degree and pattern of CC involvement, with PPMS showing predominant loss of streamlines related to the occipito-temporal regions and SPMS showing additional involvement of the motor and premotor regions. Loss of the integrity in the posterior portion of CC was the main feature of CI patients. The different spatial pattern of CC involvement observed in the two MS phenotype might be related to a different lesion load and distribution and might be associated to different pattern of grey matter atrophy. The reduced number of streamlines passing through the central and anterior portions of CC, which likely results in altered communication between the motor and prefrontal regions of the two hemispheres, was reflected in both motor disability and physical/psychosocial fatigue.Acknowledgements
This study was supported in part by the National Multiple Sclerosis Society (NMSS RG 5120A3/1).References
[1] M. Wahl, A. Hübers A, B. Lauterbach-Soon, E. Hattingen, P. Jung, L. G. Cohen, U. Ziemann. Motor callosal disconnection in early relapsing-remitting multiple sclerosis. Hum Brain Mapp. 2011;32:846-55.
[2] M. Bester, M. Lazar, M. Petracca, J.S. Babb, J. Herbert, R. I. Grossman, M. Inglese M. Tract-specific white matter correlates of fatigue and cognitive impairment in benign multiple sclerosis. J Neurol Sci. 2013;330:61-6.
[3] B. Bodini, M. Cercignani, Z. Khaleeli, D. H. Miller, M. Ron, S. Penny, A. J. Thompson, O. Ciccarelli. Corpus callosum damage predicts disability progression and cognitive dysfunction in primary-progressive MS after five years. Hum Brain Mapp. 2013;34:1163-72.
[4] R. E. Smith, J.-D. Tournier, F. Calamante, A. Connelly. Anatomically-constrained tractography: Improved diffusion MRI streamlines tractography through effective use of anatomical information. NeuroImage, 2012, 62, 1924-1938.
[5] J.-D. Tournier, F.; Calamante, A. Connelly. Improved probabilistic streamlines tractography by 2nd order integration over fibre orientation distributions. Proceedings of the International Society for Magnetic Resonance in Medicine, 2010, 1670.
Figures