3151
Evolution of functional and structural connectivity of cognitive frontoparietal network during 2 years of fingolimod therapy of multiple sclerosis1Radiology, Cleveland Clinic, Cleveland, OH, United States, 2Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH, United States, 3Neurology, Cleveland Clinic, Cleveland, OH, United States
Synopsis
It has been
reported that the cognitive impairment in MS is related to the dysfunction of frontoparietal
network (FPN). In a longitudinal study of MS patients undergoing fingolimod
treatment, we investigated the structural and function connectivity of FPN over
2 years. The trend of changes in functional connectivity MRI, and transverse
diffusivity measured by DTI probabilistic tractography indicate that fingolimod
treatment stabilized damage of structural and functional connectivity of FPN
sometime around/after the 1st year of treatment similar to that reported for
motor network.
Introduction
The oral drug fingolimod has been reported to reduce
relapse rate in patients with relapsing remitting multiple sclerosis (RRMS).1 It has been
reported that structural and functional connectivity impairment of the motor
network, as measured by diffusion tensor imaging (DTI) and functional
connectivity (fcMRI) respectively, stabilize after one year of fingolimod
treatment.2 While motor
impairment is a common symptom,3,4 cognitive
impairment is also prevalent in MS.3-5
The frontoparietal network (FPN) regulates
cognitive control,6-8
and cognitive impairment in MS has been reported to be related to the
dysfunction of the FPN.9-11
In a longitudinal study of MS patients undergoing fingolimod treatment, we investigated the FPN over 2 years by following
evolution of (i) white matter integrity (as measured by transverse diffusivity
(TD), the most relevant DTI metric in MS2,12) along a pathway between right
middle frontal gyrus (rMFG) and right inferior parietal lobule (rIPL) –
integral parts of FPN13-15 and (ii) fcMRI
between rMFG and rIPL. Cognitive performance scores, were tracked by paced
auditory serial addition test (PASAT)16
and symbol digit modalities test (SDMT).17
Methods
Twenty five MS patients (42.0±8.6 y, 80% white, 60% female) were scanned following an IRB approved protocol at 3T at baseline and 6, 12, 18 and 24 months after start of fingolimod treatment. The whole body Siemens scanner was upgraded from Tim Trio to Prisma (Erlangen, Germany) during the study; the upgrade was associated with a change of receive coil from 12 channel head coil to 20 channel (16 head + 4 spine) coil. DTI was acquired with high angular resolution diffusion imaging protocol (2mm isotropic, 71 diffusion-weighting gradients with b=1000sec/mm2 and 8 b=0 volumes, NEX=4). fcMRI data were acquired with a 2D GRE echo planar scan (TR/TE=2800/29 ms, 31 slices, slice thickness 4mm, no gap, 128×128 matrix, 256mm × 256mm FOV, bandwidth 1954 Hz/pixel, 6/8 partial Fourier, 137 repetitions). Pulse plethysmograph and respiratory bellows were used to monitor physiologic fluctuations. During fcMRI scans a bite bar was used to minimize motion and all subjects were instructed to keep eyes closed. fcMRI data analysis comprised of: (i) physiologic noise correction using RETROICOR,18 (ii) retrospective motion correction using SLOMOCO19 (iii) 2d spatial filtering in Fourier domain, followed by temporal filtering to remove all fluctuations above 0.08 Hz20, (iv) picking rMFG based upon maximum correlation with rIPL using InstaCorr routine of AFNI and creating 9 voxel rMFG and rIPL ROIs, (v) creating whole brain correlation map with rMFG voxel as seed, and (vi) computing the mean correlation within the rIPL ROI from the map. DTI analysis consisted of (i) motion correction,21 (ii) voxel by voxel tensor calculation accounting for noise floor correction,22 (iii) fiber orientation distribution23 calculation for probabilistic tractography.24,29 TD along the track connecting rMFG and rIPL (seed and target ROIs respectively, as identified from InstaCorr) was calculated. A simple random effect mixed models in GLIMMIX procedure examined time/visit effect while accounting for correlation within same patient,25 using which patterns of change of PASAT and SDMT scores over 24 months were determined. Analyses of fcMRI and DTI measures across time were done using multilevel models in GLIMMIX25 to account for scanner upgrade. Overall change (test for trend) and change over the 1st and the 2nd years were estimated based upon several contrast structures set in analyses (SAS v9.4). Two-sided p < 0.05 was considered as statistically significant.Results and Discussion
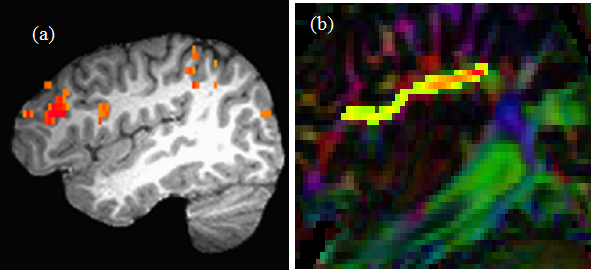
Representative images of single subject fcMRI
map and frontoparietal tracking image are shown in Fig. 1(a) and (b)
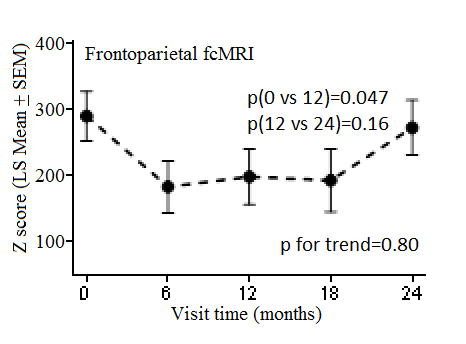
respectively. Although fcMRI did not change significantly between baseline to
24 months, it decreased significantly during the 1st year and went
back up (albeit not significantly) from 1st year to 2nd year
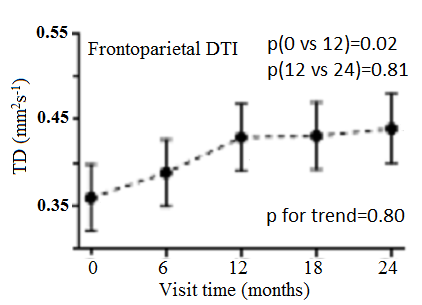
of treatment (Fig. 2). Overall TD increased over 2 years (P=0.06), while the
increase was significant during the 1st year, following which TD
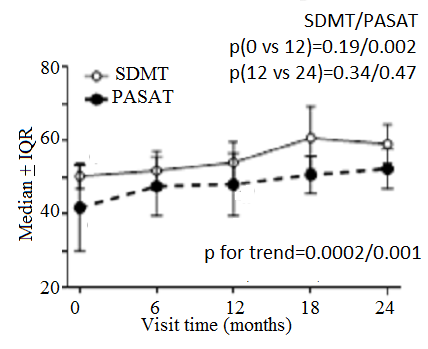
stabilized (Fig. 3). Both PASAT and SDMT scores showed overall improvement over
24 months, with PASAT performance showing significant improvement during the 1st
year (Fig. 4). While the improvement in PASAT scores may have a component of
practice effect, which has been reported to improve performance in PASAT,26, 27
such effect is minimal in SDMT28.
No correlation between overall changes in PASAT/SDMT with TD/fcMRI was
observed. Conclusion
The trend of changes in TD/fcMRI indicate that
fingolimod treatment stabilized damage of structural and functional
connectivity of frontoparietal (cognitive) network sometime around/after the 1st
year of treatment similar to that reported for motor network.2 Acknowledgements
We gratefully acknowledge funding from Novartis. We thank Thorsten Feiweier of Siemens Healthineers for developing the DTI pulse sequence and the monopolar+ functionality that was used in this study.References
1. Sanford M. Fingolimod: a review of its use in relapsing-remitting multiple sclerosis. Drugs. 2014;74(12):1411-1433.
2. Bhattacharyya PK, Fox R, Li H, Lin J, Sakaie KE, Lowe MJ. Evolution of functional and structural connectivity of motor network during 2 years of fingolimod therapy for multiple sclerosis. Proc. Intl. Soc. Mag. Reson. Med. 2018;26:1982.
3. Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372(9648):1502-1517.
4. Benedict RHB, Holtzer R, Motl RW, Foley FW, Kaur S, Hojnacki D, Weinstock-Guttman B. Upper and Lower Extremity Motor Function and Cognitive Impairment in Multiple Sclerosis. Journal of the International Neuropsychological Society. 2011;17(4):643-653.
5. Chiaravalloti ND, DeLuca J. Cognitive impairment in multiple sclerosis. Lancet Neurology. 2008;7(12):1139-1151.
6. Zanto TP, Gazzaley A. Fronto-parietal network: flexible hub of cognitive control. Trends Cogn Sci. 2013;17(12):602-603.
7. Dosenbach NUF, Fair DA, Cohen AL, Schlaggar BL, Petersen SE. A dual-networks architecture of top-down control. Trends in Cognitive Sciences. 2008;12(3):99-105.
8. Cole MW, Reynolds JR, Power JD, Repovs G, Anticevic A, Braver TS. Multi-task connectivity reveals flexible hubs for adaptive task control. Nature Neuroscience. 2013;16(9):1348-U1247.
9. Meijer KA, Eijlers AJC, Douw L, Uitdehaag BMJ, Barkhof F, Geurts JJG, Schoonheim MM. Increased connectivity of hub networks and cognitive impairment in multiple sclerosis. Neurology. 2017;88(22):2107-2114.
10. Cruz-Gomez AJ, Ventura-Campos N, Belenguer A, Avila C, Forn C. The link between resting-state functional connectivity and cognition in MS patients. Multiple Sclerosis Journal. 2014;20(3):338-348. 11. Morgen K, Sarnmer G, Courtney SM, Wolters T, Melchior H, Blecker CR, Oschmann P, Kaps M, Vaitl D. Distinct mechanisms of altered brain activation in patients with multiple sclerosis. Neuroimage. 2007;37(3):937-946.
12. Lowe MJ, Horenstein C, Hirsch JG, Marrie RA, Stone L, Bhattacharyya PK, Gass A, Phillips MD. Functional pathway-defined MRI diffusion measures reveal increased transverse diffusivity of water in multiple sclerosis. Neuroimage. 2006;32(3):1127-1133.
13. He BJ, Snyder AZ, Vincent JL, Epstein A, Shulman GL, Corbetta M. Breakdown of functional connectivity in frontoparietal networks underlies behavioral deficits in spatial neglect. Neuron. 2007;53(6):905-918.
14. Kong LT, Chen KY, Tang YQ, Wu F, Driesen N, Womer F, Fan GG, Ren L, Jiang WY, Cao Y, Blumberg HP, Xu K, Wang F. Functional connectivity between the amygdala and prefrontal cortex in medication-naive individuals with major depressive disorder. Journal of Psychiatry & Neuroscience. 2013;38(6):417-422.
15. Ptak R. The Frontoparietal Attention Network of the Human Brain: Action, Saliency, and a Priority Map of the Environment. Neuroscientist. 2012;18(5):502-515.
16. Gronwall DMA. Paced Auditory Serial-Addition Task - Measure of Recovery from Concussion. Perceptual and Motor Skills. 1977;44(2):367-373.
17. Smith A. Symbol Digits Modalities Test: Manual. West Psychol Sci. 1982:Los Angeles Western Psychological Services.
18. Glover GH, Li TQ, Ress D. Image-based method for retrospective correction of physiological motion effects in fMRI: RETROICOR. Magn Reson Med. 2000;44(1):162-167.
19. Beall EB. SimPACE: generating simulated motion corrupted BOLD data with synthetic-navigated acquisition for the development and evaluation of SLOMOCO: a new, highly effective slicewise motion correction.Neuroimage 2014 Nov 1;101:21-34. doi: 10.1016/j.neuroimage.2014.06.038. Epub 2014 Jun 24
20. Lowe MJ, Mock BJ, Sorenson JA. Functional connectivity in single and multislice echoplanar imaging using resting-state fluctuations. Neuroimage. 1998;7(2):119-132.
21. Sakaie KE, Lowe MJ. Quantitative assessment of motion correction for high angular resolution diffusion imaging. Magn Reson Imaging. 2010;28(2):290-296.
22. Sakaie K, Lowe M. Retrospective correction of bias in diffusion tensor imaging arising from coil combination mode. Magn Reson Imaging. 2017;37:203-208.
23. Sakaie KE, Lowe MJ. An objective method for regularization of fiber orientation distributions derived from diffusion-weighted MRI. Neuroimage. 2007;34(1):169-176.
24. Lowe MJ, Beall EB, Sakaie KE, Koenig KA, Stone L, Marrie RA, Phillips MD. Resting state sensorimotor functional connectivity in multiple sclerosis inversely correlates with transcallosal motor pathway transverse diffusivity. Hum Brain Mapp. 2008;29(7):818-827.
25. Brown H, Prescott R. Applied Mixed Models in Medicine. Norwood, MA: Artech Hhouse; 1999.
26. Barker-Collo SL. Within session practice effects on the PASAT in clients with multiple sclerosis. Arch Clin Neuropsychol. 2005;20(2):145-152.
27. Bever CT, Jr., Grattan L, Panitch HS, Johnson KP. The Brief Repeatable Battery of Neuropsychological Tests for Multiple Sclerosis: a preliminary serial study. Mult Scler. 1995;1(3):165-169.
28. Benedict RH, Duquin JA, Jurgensen S, Rudick RA, Feitcher J, Munschauer FE, Panzara MA, Weinstock-Guttman B. Repeated assessment of neuropsychological deficits in multiple sclerosis using the Symbol Digit Modalities Test and the MS Neuropsychological Screening Questionnaire. Mult Scler. 2008;14(7):940-946.
29. Zhang, M (2013) ”Logical Foundations and Fast Implementation of Probabilistic Tractography” IEEE Trans Med Imaging. Aug;32(8):1397-410. doi 10.1109/TMI.2013.2257179
Figures