3150
Combining Structural and Functional Connectivity as Biomarkers for Disease Progression in Neurologic Disease: A Longitudinal Multiple Sclerosis Study1Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 2Biomedical Engineering, Cleveland Clinic, Cleveland, OH, United States, 3Neurologic Institute, Cleveland Clinic, Cleveland, OH, United States
Synopsis
Sensitive outcome measures are required to test novel therapies designed to target neurodegeneration in Multiple Sclerosis(MS). We have previously shown that functional connectivity using resting-state fMRI (rs-fMRI) and anatomic connectivity using DTI are related in the transcallosal motor pathway and along the memory pathway connecting hippocampus to posterior cingulate. We propose a combined metric incorporating anatomic and functional connectivity along these pathways as a potential biomarker of disease progression in MS. In this study, we present results from a 2 year study that assessed this biomarker in 19 MS patients at six timepoints. We show that our metric is sensitive to changes in MS disease over this time interval. We also show that our metric is more sensitive to change than typically used imaging biomarkers.
Introduction
We have previously shown that functional connectivity using resting-state fMRI (rs-fMRI) and anatomic connectivity using DTI are related in the transcallosal motor pathway and along the memory pathway connecting hippocampus (Hipp) to posterior cingulate (PCC)(1, 2). We propose a combined metric incorporating anatomic and functional connectivity along these pathways as a potential biomarker of disease progression in MS. In this study, we present results from a 2 year study that assessed this biomarker in 19 MS patients at six timepoints. We show that our metric is sensitive to changes in MS disease over this time interval.Methods
AIFCI: Our metric, the anatomic impairment
functional connectivity index (AIFCI), is the sum of z-scored measures of
pathway-dependent DTI and RS-fMRI measures. Radial diffusivity (RD), based on
Lowe et al.(2),
is a good measure of anatomic connectivity in the pathways of interest here.
Two systems are assessed: the motor system and the episodic memory system. We
take the z-score corrected Student t (3)
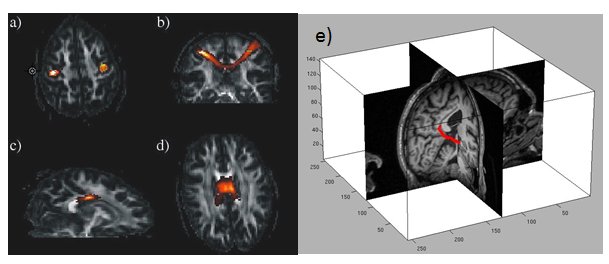
as our measure of functional connectivity, fc.RD and fc are assessed in the transcallosal motor pathway (SMC) and the posterior cingulate to entorhinal cortex pathway (PCC-ENT), bilaterally. The latter pathway constitute the posterior part of the cingulum bundle, or the Papez circuit, known to be involved in episodic memory.
Motor AIFCI measure: The motor AIFCI is calculated according to: $$Z_{motor}=\frac{1}{2}[\frac{(f_c-f_{c}^{pop})}{\sigma_{c}^{pop}}-\frac{(RD-RD^{pop})}{\sigma_{RD}^{pop}}]$$
$$$f_c^{pop}$$$, $$$\sigma_c^{pop}$$$ and $$$RD^{pop}$$$, $$$\sigma_{RD}^{pop}$$$ can be either population or sample means and standard deviations. The metric is constructed such that the measure will decrease with increased disability.
Memory AIFCI measure: Because the PCC-ENT pathway is intrahemispheric and bilateral, the memory AIFCI measure, $$$Z_{memory}$$$, is constructed similarly to the motor Z, but separately for each hemisphere
Finally, component Z's are combined in the following manner:
$$AIFCI=\frac{1}{2}Z_{motor}+\frac{1}{2}MIN[Z_{memory}^L,Z_{memory}^R]$$
Data Acquisition: Nineteen MS patients (age: 51.1 ± 7.0yrs,6 male, EDSS: 4.1[2-6.5])were scanned at 6 timepoints over 2 years. Ten age and sex matched healthy controls (age: 48.4± 7.2yrs, 3 male) were scanned at baseline and 2 years. Imaging data were acquired on a Siemens 3T MRI scanner (Erlangen, Germany). High resolution T1 and T2 weighted images were acquired for display and structural analyses described below. HARDI data were acquired: (TE/TR=102/7700msec, 128x128x48 matrix, FOV=256x256x96mm), 71 b=1000 sec/mm2 acquisitions, and 8 b=0 acquisitions. Motion correction was performed using FSL(6). Resting state scan: 132 repetitions of 31-4mm thick axial slices acquired with TE/TR=29ms/2800 ms, 128x128 matrix, 256mm x 256mm FOV, receive bandwidth=1954Hz/pixel. Motion correction is performed using SLOMOCO(4)
Structural measures: Measures of brain parenchymal fraction (BPF) and T2-weighted lesion volumes (T2LV) were analyzed using semi-automated software(5).
Group Level Analysis: For each AIFCI measure, analyses were performed using linear mixed effects regression (LMER)(6). Data from both patients and controls at baseline and the final session were entered into a LMER analysis. “Group” was entered as an ordered variable (healthy control or patient). Linear effects of time were tested using session, and a group x time interaction was included. A reduced model (omitting group) was compared to the full model using the likelihood ratio test (LRT). The false discovery rate adjustment (FDR) was applied.
Results
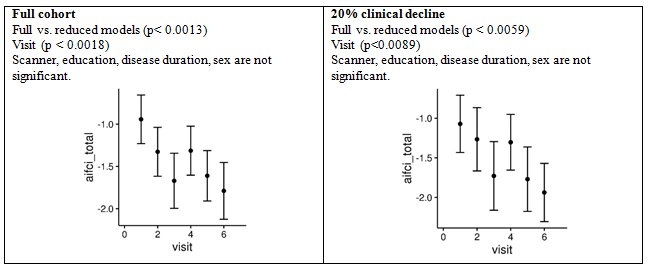
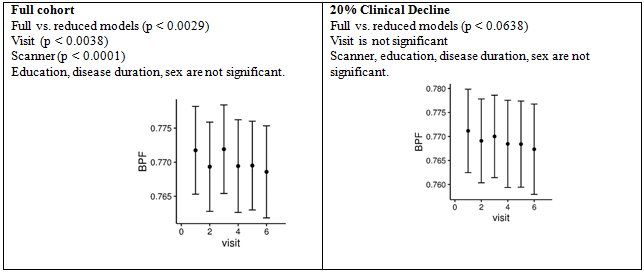
Figure 2 shows the AIFCI calculated for each visit for all patients and for those with 20% clinical decline (11 patients). As shown, the AIFCI shows a pronounced decline across the two years and our model shows significance for group as well as visit, demonstrating that AIFCI is sensitive to disease progression over the duration of the study. Figure 3 shows the same analyses, only for BPF. BPF does not demonstrate the same decline nor the same level of significance for either group or visit. Importantly, BPF is not significant for either group or visit in the cohort that demonstrated clinical decline over the two years, while AIFCI is significant for both. Lesion volume analyses were not significant for either group or visit.Discussion and Conclusion
We demonstrate that an imaging metric based on structural and functional connectivity in motor and cognitive pathways in the brain is sensitive to disease progression in MS. In this study, our metric was more sensitive over time and in comparison to healthy controls than either BPF or lesion volume analyses. We suggest that AIFCI may be an effective biomarker for drug therapy development in MS.Acknowledgements
This study was funded by a grant from the National Multiple Sclerosis Society.References
1. Lowe MJ, Beall EB, Sakaie KE, Koenig KA, Stone L, Marrie RA, Phillips MD. Resting state sensorimotor functional connectivity in multiple sclerosis inversely correlates with transcallosal motor pathway transverse diffusivity. Human brain mapping. 2008;29(7):818-27. PubMed PMID: 18438889.
2. Lowe MJ, Koenig KA, Beall EB, Sakaie KA, Stone L, Bermel R, Phillips MD. Anatomic connectivity assessed using pathway radial diffusivity is related to functional connectivity in monosynaptic pathways. Brain connectivity. 2014;4(7):558-65. PubMed PMID: 25117651.
3. Lowe MJ, Mock BJ, Sorenson JA. Functional connectivity in single and multislice echoplanar imaging using resting-state fluctuations. NeuroImage. 1998;7(2):119-32.
4. Beall EB, Lowe MJ. SimPACE: Generating simulated motion corrupted BOLD data with synthetic-navigated acquisition for the development and evaluation of SLOMOCO: A new, highly effective slicewise motion correction. NeuroImage. 2014;101:21-34. PubMed PMID: 24969568.
5. Fisher E, Rudick RA, Cutter G, Baier M, Miller D, Weinstock-Guttman B, Mass MK, Dougherty DS, Simonian NA. Relationship between brain atrophy and disability: an 8-year follow-up study of multiple sclerosis patients. Multiple sclerosis (Houndmills, Basingstoke, England). 2000;6(6):373-7. doi: 10.1177/135245850000600602. PubMed PMID: 11212131.
6. Bates M, Machler M, Bolker B, Walker S. Fitting Linear Mixed-Effects Models Using lme4. Journal of Statistical Software. 2015;67(1):1-48.
Figures