3144
Characterization of gray-matter multiple sclerosis lesions using double inversion recovery, diffusion, contrast-enhanced, and volumetric MRI1Radiology, Stony Brook University Hospital, Stony Brook, NY, United States, 2Stony Brook University, Stony Brook, NY, United States, 3Neurology, Stony Brook University Hospital, Stony Brook, NY, United States
Synopsis
This study characterized gray-matter (GM) multiple sclerosis (MS) lesions using double-inversion recovery (DIR), contrast-enhanced and diffusion at 3T MRI. Lesion segmentation was based on DIR. We determined GM lesion prevalence, characterize their contrast-enhancement and diffusion characteristics, and compared them with white-matter (WM) lesions. Correlated GM lesion count and volume with total brain, WM, GM and deep GM volumes, as well as clinical disability. Comparisons were also made with healthy controls. We tested the hypothesis that GM MS lesions are highly prevalent, contrast-enhanced GM lesions have higher ADC values, and GM MS lesion counts and volumes are correlated with brain atrophy.
Introduction
Gray-matter (GM) lesions in multiple sclerosis (MS) have been shown to correlate with the severity of physical disability and cognitive impairment compared to white-matter (WM) lesions1,2. In the 2017 revised McDonald diagnostic criteria, GM lesions was added as a preferred lesion site as MRI criteria for MS diagnosis3, underscoring the importance of GM damage in MS. While WM lesions are well studied in multiple sclerosis (MS), GM lesions are not well studied because they are non-conspicuous on conventional MRI. Double-inversion recovery (DIR) has recently been shown to improve detection of GM lesions when compared to FLAIR4. Diffusion-weighted imaging (DWI) and contrast-enhanced MRI have been extensively used to characterize WM lesions5,6, but similar studies characterizing GM lesions are sparse. Histopathological and immunological data further suggest that there are significant differences in pathophysiology between GM and WM MS lesions7,8. DWI and contrast-enhanced MRI may prove useful for characterizing GM MS lesions in vivo in clinical settings. This study characterized GM MS lesions using DIR, contrast-enhanced and diffusion at 3T MRI. We also compared GM lesions to WM, and correlated GM lesions to brain atrophy. We tested the hypothesis that GM lesions are contrast-enhanced with similar prevalence as WM lesions, contrast-enhanced GM lesions have higher ADC values, and GM MS lesion counts and volumes are correlated with brain atrophy.Methods
3T MRI data for this retrospective study included T1WI, DIR, FLAIR, and DWI. We analyzed 44 RRMS patients (12M/32F, 41±13yo, disease duration 7±7) and 24 age-matched healthy controls (14M/10F, 36±13yo). Lesions were manually segmented based on DIR and grouped into GM, subcortical WM, and periventricular WM lesions. ADC were tabulated for contrast-enhancing and non-enhancing lesions. Brain volume segmentation performed using FSL SIENAX and FIRST, volumes adjusted for age and brain size. Unpaired single t-tests were used for comparison between groups. Linear regression was used to evaluate the relationship between number of GM lesions and total GM lesion volume with brain volumes and clinical data.Results
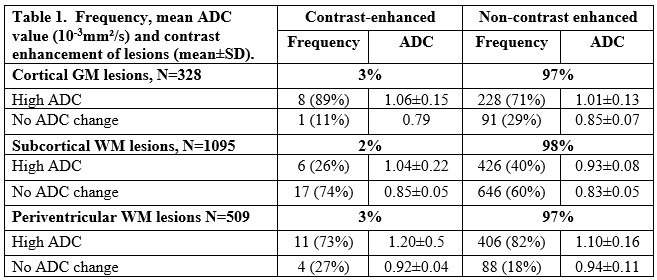
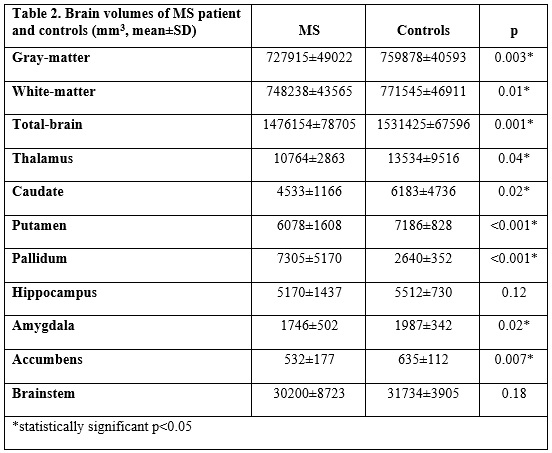
We found a total of 1931 lesions, 94% were hyperintense on both FLAIR and DIR. In our cohort, 86% of patients had GM lesions. 328 GM lesions were identified, 3% of which was contrast-enhanced. 1095 subcortical WM lesions, 2% was enhanced. 509 periventricular WM lesions, 3% enhanced (Table 1). Differences in brain volumes were found between patients and controls (Table 2). Number of GM lesions significantly correlated with decreasing GM and total-brain (TB) volume (p<0.004 and p<0.005, respectively), but not with WM volume or deep GM structures. GM lesion volume correlated with decreasing GM, WM, TB and putamen volume (p=0.01, p=0.04, p=0.006 and p=0.01, respectively). We dichotomized our patients into less severe (<5s) and more severe (≥5s) disability based on 25-foot walk test. The more severe disability group showed lower volumes when compared to the less severe group in thalamus (p=0.01), caudate (p=0.001), putamen (p=0.002), hippocampus (p=0.007), amygdala (p=0.007), accumbens (p=0.003) and brainstem (p=0.03), but no significant differences in GM, WM, TB and pallidum volume (p>0.05).Discussion
In our cohort, 86% of our patients had GM lesions on DIR at 3T MRI, this is in line with other studies9,10. However, these studies did not investigate ADC of GM lesions nor correlate GM lesions with brain atrophy. The percentage of enhancing lesions were similar for both GM and WM, suggesting that loss of blood-brain barrier integrity is similar, our results could also be explained that we included both intracortical and juxtacortical lesions, but further studies are needed to make a conclusion. GM lesion counts strongly correlated with GM and TB atrophy. GM lesion volumes strongly correlated with GM, WM, TB and putamen atrophy. We also see more pronounced deep GM structures atrophy in patients that have more severe disabilities. Our patients have relatively mild disease, per disease duration, but we can see that GM lesions play an important role in brain atrophy. GM lesion correlation is an area that still remains to be explored, the few studies out there have inconsistent results9,11. Future studies should include, longitudinal follow up with additional MRI measures as well as correlation with neuropsychology tests.Conclusion
GM MS lesions are present in the majority of MS patients, supporting the notion that GM damage plays an important role in MS pathogenesis. GM lesion count and volume correlate with brain atrophy. Patients with more severe disability as measured with the 25 foot-walk test, show lower brain volumes in the deep GM. Identifying early GM changes and understanding of GM lesion MRI-pathophysiology in vivo may prove useful for management of the disease including improving targeted therapy and monitoring of disease progression.Acknowledgements
NoneReferences
1. Calabrese M, Agosta F, Rinaldi F, Mattisi I, Grossi P, Favaretto A, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(9):1144-50.
2. Calabrese M, De Stefano N, Atzori M, Bernardi V, Mattisi I, Barachino L, et al. Detection of cortical inflammatory lesions by double inversion recovery magnetic resonance imaging in patients with multiple sclerosis. Arch Neurol. 2007;64(10):1416-22.
3. Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 2018;17(2):162-73.
4. Geurts JJ, Pouwels PJ, Uitdehaag BM, et al. Intracortical lesions in multiple sclerosis: improved detection with 3D double inversion-recovery MR imaging. Radiology 2005;236(1):254-60.
5. Castriota Scanderbeg A, Tomaiuolo F, Sabatini U, Nocentini U, Grasso MG, Caltagirone C. Demyelinating plaques in relapsing-remitting and secondary-progressive multiple sclerosis: assessment with diffusion MR imaging. AJNR. 2000;21(5):862-8
6. Roychowdhury S, Maldjian JA, Grossman RI. Multiple sclerosis: comparison of trace apparent diffusion coefficients with MR enhancement pattern of lesions. AJNR. 2000;21(5):869-74.
7. Bo L, Vedeler CA, Nyland H, Trapp BD, Mork SJ. Intracortical multiple sclerosis lesions are not associated with increased lymphocyte infiltration. Mult Scler. 2003;9(4):323-31.
8. Geurts JJ, Bo L, Pouwels PJ, Castelijns JA, Polman CH, Barkhof F. Cortical lesions in multiple sclerosis: combined postmortem MR imaging and histopathology. AJNR. 2005;26(3):572-7.
9. Ertan G AO, Ulus S, Metin B. Efficiency of double inversion recovery (DIR) sequence in the evaluation of supratentorial cortical lesions in multiple sclerosis. Neuroquantology 2018;16(3):23-9.
10. Kolber P, Montag S, Fleischer V, et al. Identification of cortical lesions using DIR and FLAIR in early stages of multiple sclerosis. J Neurol 2015;262(6):1473-82.
11. Harrison DM, Roy S, Oh J, et al. Association of Cortical Lesion Burden on 7-T Magnetic Resonance Imaging With Cognition and Disability in Multiple Sclerosis. JAMA Neurol 2015;72(9):1004-12.
Figures