3139
Multimodal 7T MRI of epilepsy surgery candidates: Prospective evaluation of impact on presurgical decisionsGiske Opheim1,2, Melanie Ganz-Benjaminsen1,3, Patrick Fisher1, Ulrich Lindberg4, Mark Bitsch Vestergaard4, Helle Juhl Simonsen4, Henrik Bo Wiberg Larsson4, Anne-Mette Leffers5, Camilla Gøbel Madsen5, Olaf Bjarne Paulson1, and Lars Hageman Pinborg1,2
1Neurobiology Research Unit, Dept. of Neurology, Rigshospitalet, Copenhagen, Denmark, 2Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark, 3Dept. of Computer Science, University of Copenhagen, Copenhagen, Denmark, 4Functional Imaging Unit, Dept. of Clinical Physiology, Nuclear Medicine and PET, Rigshospitalet - Glostrup, Copenhagen, Denmark, 5Dept. of Diagnostic Radiology, Centre for Functional & Diagnostic Imaging and Research, Hvidovre Hospital, Copenhagen, Denmark
Synopsis
Identifying lesions at 3T MRI remains the most important correlate to epilepsy surgery outcome. Since 45% of candidates present with negative 3T MRI, investigation of diagnostic yield of clinical 7T MR protocols along with post-processing markers is urged. This ongoing study will evaluate how radiological descriptions and computational morphometrics affect presurgical decisions. So far, 19 patients and 31 controls are scanned at the Philips Achieva 7T system at Hvidovre Hospital, Denmark. Preliminary analyses of automatic segmentations show promising potential. We are in radiological training, but expect first case with evaluation of impact on presurgical decision to start around new-year 2018/2019.
Introduction
Identification of an epileptogenic lesion on MRI at conventional field strengths is considered the most important correlate of surgical outcome1. As 45% of surgical candidates present with negative MRI, investigations of the diagnostic yield of radiological assessment of submillimeter resolution scans with higher SNR from 7T have already been published2-4. These studies vary in basis for comparison and study design, and therefore also the conclusions with regards to effect of 7T MRI on detection rates, as well as delineation details of epileptogenic lesions. Further, investigation of targeted post-processing MRI markers is urged5-6. This ongoing study will analyze the sensitivity and specificity of targeted structural 7T MR metrics as markers of the seizure focus and pathways, and prospectively evaluate their impact on decisions made about patients included in the Danish Epilepsy Surgery (DES) program.Scans and Analysis
So far, we have recruited 19 epilepsy patients and 31 healthy controls (HCs) at the Philips Achieva 7T system at Hvidovre Hospital, which was upgraded to software Release 5.1.7 before project start. The structural protocol consists of five scans (3D MPRAGE, 3D FLAIR, 3D T2, and two T2 slabs) to proximate the current 3T protocol set by DES, see Fig. 1 for T2 image examples. All scans are performed with a 32/2 Tx/Rx channel Nova Head Coil, and we use dielectric pads to adjust for field imhomogeneities. Scan duration is 55 minutes, due to an additional functional MRI protocol.Here, we can present preliminary analysis of cortical thickness- and hippocampal subfield segmentations in Freesurfer 6.0 (Fig. 2). All computations are done for both 7T and 3T data. They are based on 3D T1-images, and for hippocampal subfield segmentation, also on an overlay with the 3D T2-images. The 3D T1-weighted images from 7T are subjected to bias field correction prior to cortical reconstructions, in order to assure high quality of the surface reconstructions. The radiological assessment is performed by two experienced neuro-radiologists who are specialized in epilepsy pathology.
Results
The computational results have been assessed for 15 single patients so far. Results for 7T and 3T hippocampal subfield segmentation concur for patients with mesial temporal sclerosis (MTS) diagnosis (Fig. 3), though 7T results seem more sensitive. We are still in the radiological training process, but some preliminary visual assessments have been made. E.g, patient 5, a patient with right-sided polymicrogyria as the only clinical finding on 3T MRI, displays hippocampal asymmetry with all right subfields and whole right hippocampus being larger than the left on the 7T image, while only certain subfields (but not whole hippocampal volume) display significant asymmetry on the 3T image. Hippocampal pathology was not detected during radiological assessment. Patient 10, the second case of polymicrogyria, does not display the same degree of hippocampal asymmetry for neither 7T or 3T data. Seen together, this may indicate that there is also pathology in the hippocampi/temporal lobe of patient 5, which in turn might have an impact on presurgical decisions. Results from cortical parcellations seem to display random variabilities in thickness, asymmetries between hemispheres, and 7T vs 3T differences for HCs and all patients, except patients 5 and 10, who have unilateral polymicrogyria.Conclusive remarks
These preliminary assessments demonstrate a potential for including automatically segmented cortical regions and hippocampal subfields in this epilepsy patient group. All reconstructions are performed with minimal manual correction of surfaces for both 3T and 7T data, and thus perform at a satisfactory level. This may therefore serve as basis for, e.g., automatic detection of cortical regions with significant thickness abnormalities, which is of interest during epilepsy diagnostics.Albeit the systematic radiological descriptions of 7T MR images are still on their way, our impression is that the standard and more directly comparable (to 3T) clinical scan protocol yields images of overall good quality. The current patient group is too heterogeneous, and thus the various sample sizes (patient subgroups) are yet too small to do any quantitative group comparison and explanation of 7T vs. 3T differences in thickness and volumes. We will continue the inclusion of epilepsy patients through 2020.
The first impact evaluation case with this "7T MR package" of targeted computational results together with radiological descriptions is expected to start around new-year 2018/2019.
Acknowledgements
We acknowledge the sponsors of the Danish national 7T MR project: The Danish Agency for Science, Technology and Innovation grant no. 0601-01370B, and The John and Birthe Meyer Foundation. Further, we acknowledge the continuous assistance with ad hoc scanning issues as well as finetuning of sequences from Esben Thade Petersen, Vincent Boer, Anouk Marsman (7T Core Group, Danish Research Centre for Magnetic Resonance) and Jan Ole Pedersen (Clinical MR Scientist, Philips). The project is supported by the Danish Council for Independent Research | Medical Sciences grant no. DFF-7016-00151 and by the Lundbeck Foundation grant no. R280-2017-3925.References
1. Bien, Christian G., et al. "Characteristics and surgical outcomes of patients with refractory magnetic resonance imaging–negative epilepsies." Archives of Neurology 66.12 (2009): 1491-1499.2. Veersema, Tim J., et al. "Seven tesla MRI improves detection of focal cortical dysplasia in patients with refractory focal epilepsy." Epilepsia Open 2.2 (2017): 162-171.
3. Colon, A. J., et al. "Detection superiority of 7 T MRI protocol in patients with epilepsy and suspected focal cortical dysplasia." Acta Neurologica Belgica 116.3 (2016): 259-269
4. De Ciantis, Alessio, et al. "7T MRI in focal epilepsy with unrevealing conventional field strength imaging." Epilepsia 57.3 (2016): 445-454.
5. Wang, Z. Irene, and Andreas V. Alexopoulos. "MRI Post-processing in Pre-surgical Evaluation." Current opinion in neurology 29.2 (2016): 168.
6. Whelan, Christopher D., et al. "Structural brain abnormalities in the common epilepsies assessed in a worldwide ENIGMA study." Brain 141.2 (2018): 391-408.
Figures
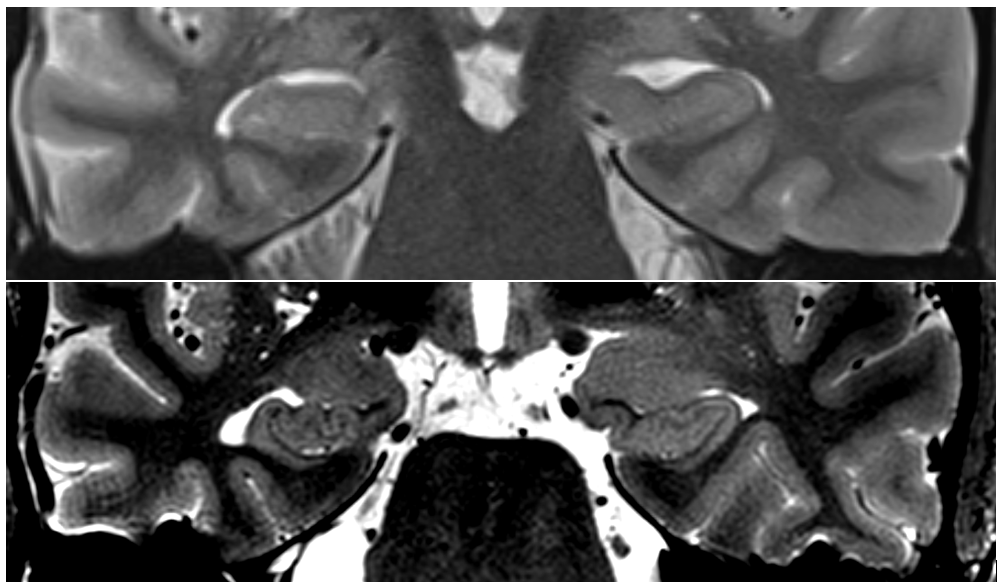
Paracoronal T2 (TSE) images of patient 14, with suspected temporal lobe epilepsy, where the quality of the T2-weighted images in the protocols are critically important for assessment of the hippocampi. The difference in structural information between 3T (top) and 7T (bottom) is evident.
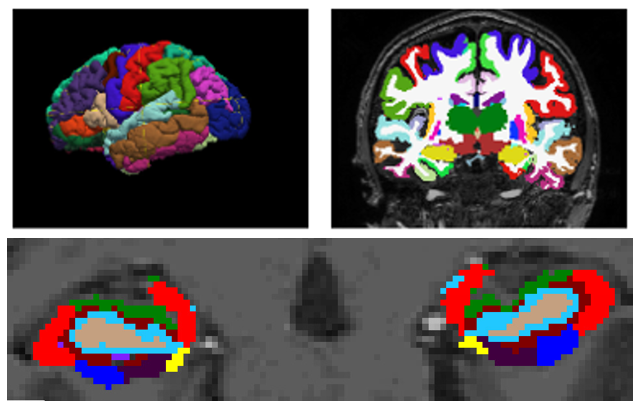
Top, 3D and coronal view of cortical parcellations based on 7T images. Bottom, Coronal view on hippocampal subfields as segmented from an overlay of 7T 3D T1- and T2 images.
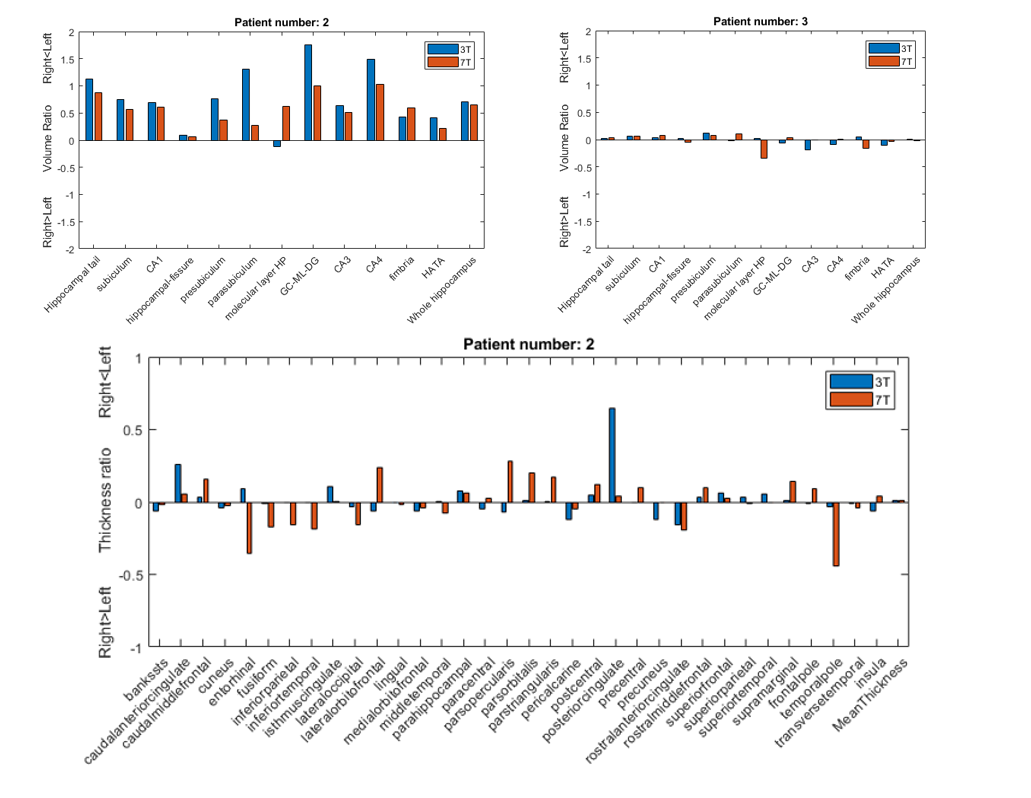
Top: Left, Example of the significant asymmetries for hippocampal subfields in one of our patients with MTS. Right, Example of unrevealing results, which is representative for all patients without MTS, except for patient 5. Bottom: Demonstration of the variability in asymmetries and disagreements between 7T and 3T for the cortical regions, representative for all patients except for patients 5 and 10.