3136
Asymmetry of hippocampus vasculature in temporal lobe epilepsy1Translational and Molecular Imaging Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Neurology, Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
Epilepsy is a chronic and prevalent disease. When epilepsy is drug resistant, resection of epileptogenic abnormalities may control seizures. However, there exist focal epileptogenic abnormalities which are not well visualized by current imaging techniques. Hippocampal vascularity has yet to be explored as an in vivo marker for the epileptic brain. Using susceptibility weighted imaging at 7T MRI we are able to visualize vessels in the hippocampus, and have automatically segmented the vessels in the hippocampus of 19 patients with temporal lobe epilepsy and 19 healthy controls. We found significant asymmetry in the vessel density in patients with epilepsy when compared against healthy controls.
Purpose
Epilepsy is a chronic condition characterized by recurrent seizures [1-5]. Temporal lobe epilepsy is a common form of the disease that is often drug-resistant and amenable to surgical intervention. Identification of structural or signal asymmetry among hippocampi on magnetic resonance imaging scans is a key indicator of a primary epileptogenic zone. However, patients may also have distinct epileptogenic abnormalities that do not correlate with focal lesions on pre-surgical imaging [6-7]. Identification of biomarkers associated with epilepsy may improve our ability to assess and treat patients with drug resistant disease. Since animal models of temporal lobe epilepsy suggest that seizures may affect the vascular network in the hippocampus [8], even without significant hippocampal asymmetry, alterations in local vessels may be an important ictal biomarker. However, to date the vascular pattern among this population has been inconsistent: some histologic reports have suggested higher hippocampal blood vessel density [9-11], while other investigations using high magnification light microscopy suggest a reduction of blood vessels in epileptogenic zones [12-13]. We hypothesized that susceptibility weighted imaging (SWI) at 7T could exploit changes caused by paramagnetic deoxygenated blood to achieve very high resolution in vivo characterization of veins which allows us to better characterize hippocampal vessels in epilepsy. We have developed a method to automatically segment vessels from SWI images and calculate localized density of vessels. We apply this to non-lesional temporal lobe epilepsy patients and calculate the asymmetry of vessels in their hippocampi.Methods
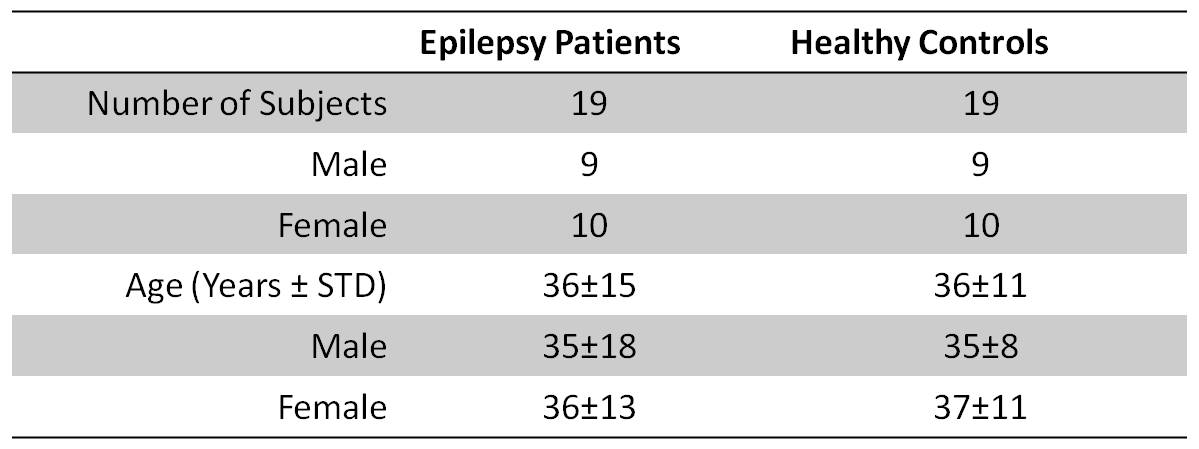
19 healthy controls and 19 patients with non-lesional focal epilepsy of suspected temporal lobe origin were scanned on a 7T MRI (Siemens, MAGNETOM) using a 32-channel head coil (Nova Medial). MP2RAGE [14] and SWI were acquired as part of a comprehensive imaging protocol (including T2 FLAIR) [15]. Institutional Review Board approval for human research was obtained for this research. Patient Demographics are listed in Figure 1.
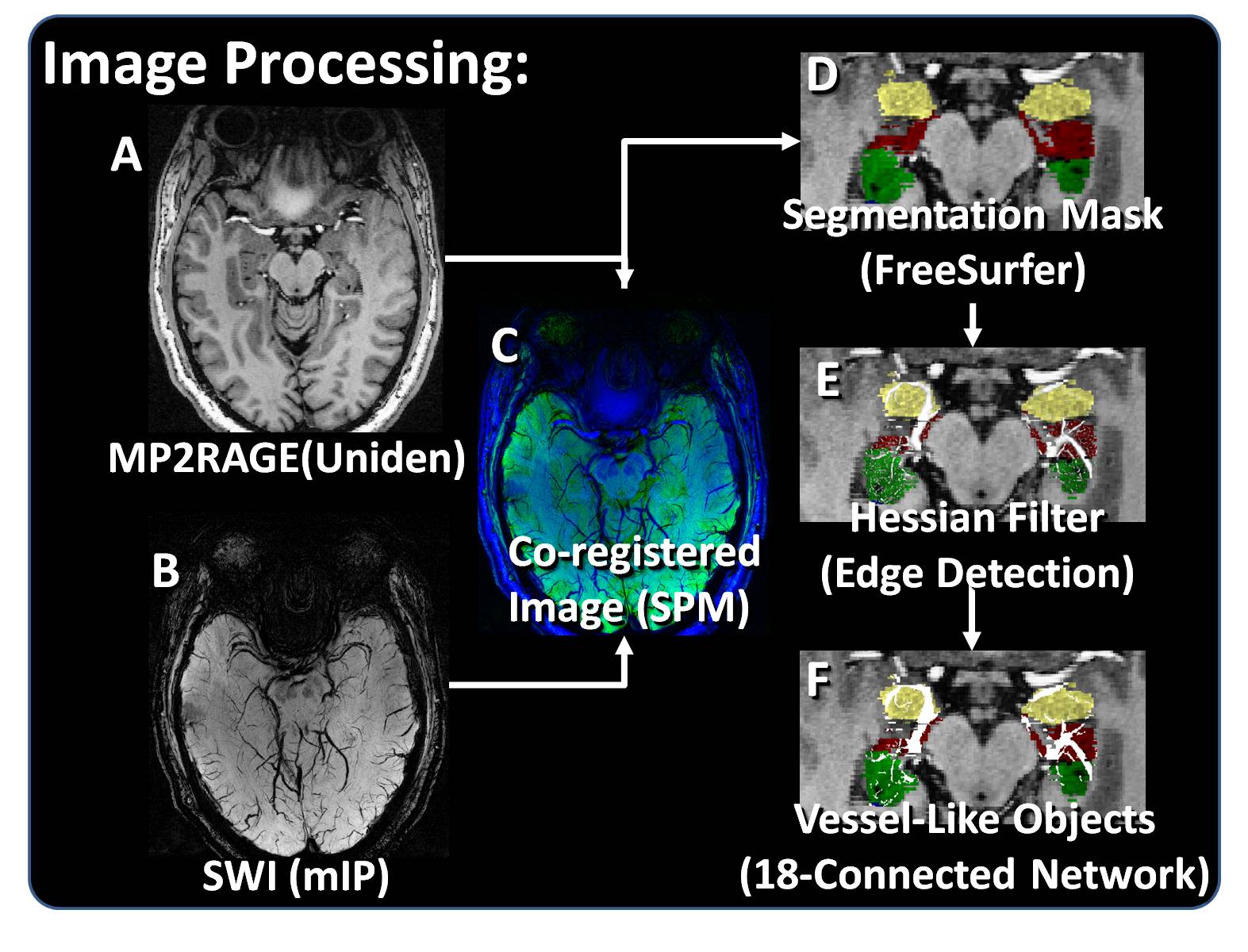
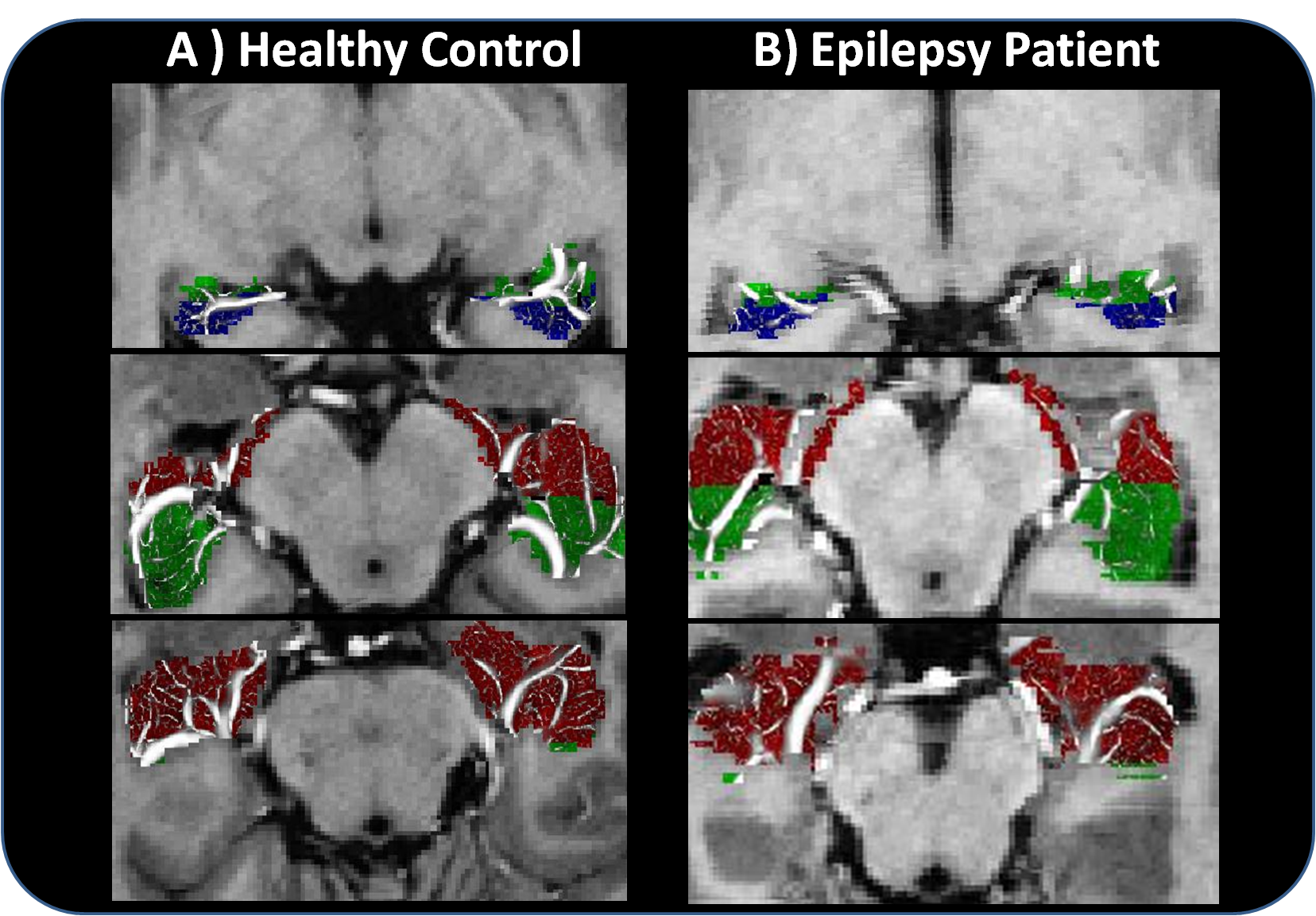
The protocol developed to detect potential venous structures from the acquired data is illustrated in Figure 2. Vessel detection was performed in MATLAB (The Mathworks, Inc, Natick, MA) using the SWI minimum intensity projection (mIP), and the segmentation masks used to isolate hippocampal vessels were created based on the UNIDEN images processed in FreeSurfer v.6.0 (http://surfer.nmr.mgh.harvard.edu, MGH). The network was thresholded to exclude objects with a connected length of less than 4 voxels. Figure 3 shows representative results for one epilepsy patient and one control.
The hippocampal volume (HV) was calculated from the voxels contained within the volumetric segmentation of the hippocampus and the vessel volume (VV) was calculated from the total number of voxels traced in each ROI scaled by the voxel volume. The vessel density was estimated by calculating the vessel volume and dividing by the hippocampal volume ($$$VD = VV/HV$$$). The symmetry of the vessel density and hippocampal volume was quantified by calculating an asymmetry index $$$|AI| = (2|R-L|)/(R+L)$$$, an unsigned value where R or L refer to right or left HV or VD in the respective regions of interest. The epilepsy patient and healthy control populations were compared using at t-test and Mood’s Median Test.
Results/Discussion
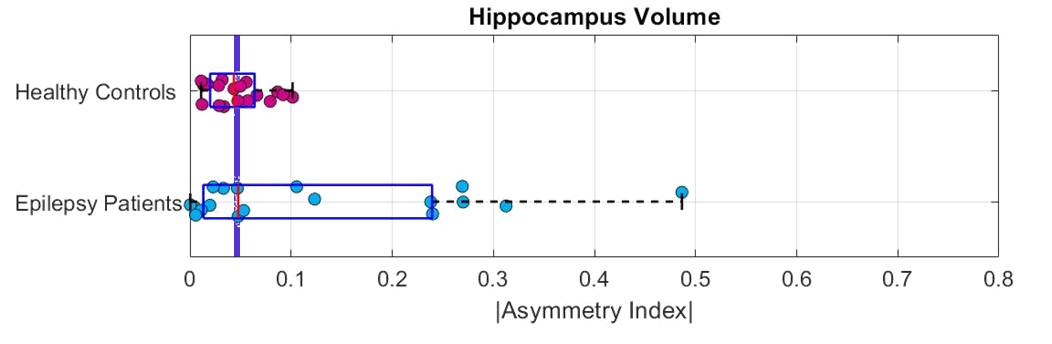
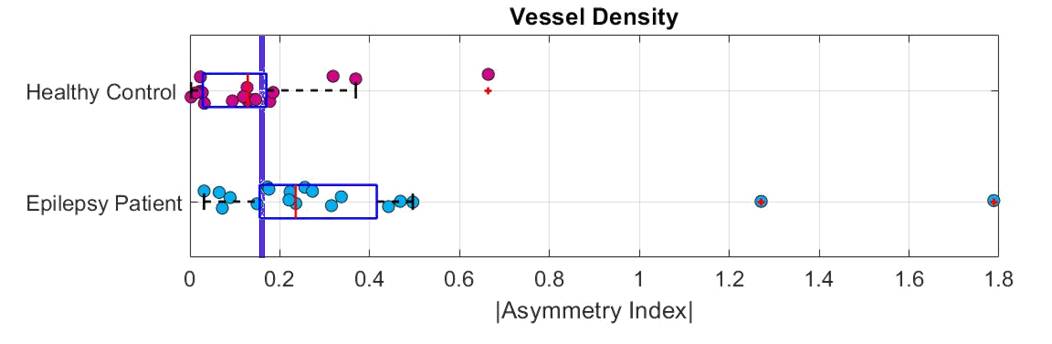
As shown in Figure 4, the mean hippocampal AI was significantly lower in healthy controls than epilepsy patients (mean |AIv| of 0.05 ± 0.03 vs 0.1 ± 0.1, p = .03). However, a Mood’s Median test of the population shows that only 10/19 healthy controls had asymmetry lower than the group mean compared to 9/19 of the epilepsy patients. This results in a χ2 = 0.11, reflecting no significant separation between the two groups and suggesting volumetric asymmetry is a poor differentiator between healthy controls and temporal lobe epilepsy. However, as shown in Figure 5, the mean vessel density AI was also lower in healthy controls compared to epilepsy patients (mean |AId| = 0.1 ± 0.1 vs. 0.4 ± 0.4, p = .04). For this metric, only 5/19 healthy controls had an |AId| larger than the median, while 14/19 epilepsy patients did, resulting in a χ2 = 8.5 and a significant separation between the two groups (p = 0.004). For example, fewer than 16% of the healthy controls had an |AId| greater than 0.2 while more than 68% of epilepsy patients did. This asymmetry is positively driven by a decrease in vessel density ipsilateral to the suspected seizure onset zone.Conclusion
Calculations of vessel density in the hippocampi of patients with temporal lobe epilepsy enabled quantification of asymmetry between the right and left hippocampus. Asymmetry in vessel density provided significant distinction between healthy controls and epilepsy patients while a significant difference in hippocampal volume did not provide the same differentiation.Acknowledgements
NIH R00 NS070821
NIH R01 MH109544
Icahn School of Medicine Capital Campaign
Translational and Molecular Imaging Institute
References
[1] Ngugi AK, Bottomley C, Kleinschmidt I, Wagner RG, Kakooza-Mwesige A, Ae-Ngibise K, Owusu-Agyei S, Masanja H, Kamuyu G, Odhiambo R, Chengo E, Sander JW, Newton CR. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies. Lancet Neurol 2013; 12: 253-263.
[2] Bell GS, Sander JW. The epidemiology of epilepsy: the size of the problem. Seizure 2001; 10: 306-314.
[3] Murray CJ, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2197-2223.
[4] WHO. Epilepsy:epidemiology, aetiology and prognosis. In Epilepsy:epidemiology, aetiology and prognosis. World Health Organization: City, 2001
[5] Belhocine; M, deBoer; H, Mandlhate C. Epilepsy in the WHO African Region: Bridging the Gap. In Epilepsy in the WHO African Region: Bridging the Gap, Editor (ed)^(eds). World Health Organization: City, 2004
[6] Duncan JS, Sander JW, Sisodiya SM, Walker MC. Adult epilepsy. Lancet 2006; 367: 1087-1100
[7] So EL. Role of neuroimaging in the management of seizure disorders. Mayo Clin Proc 2002; 77: 1251-1264
[8] Leal-Campanario R, Alarcon-Martinez L, Rieiro H, Martinez-Conde S, Alarcon-Martinez T, Zhao X, LaMee J, Popp PJ, Calhoun ME, Arribas JI, Schlegel AA, Stasi LL, Rho JM, Inge L, Otero-Millan J, Treiman DM, Macknik SL. Abnormal Capillary Vasodynamics Contribute to Ictal Neurodegeneration in Epilepsy. Sci Rep; 7: 43276.
[9] Pitkanen A, Lukasiuk K. Molecular and cellular basis of epileptogenesis in symptomatic epilepsy. Epilepsy Behav 2009; 14 Suppl 1: 16-25
[10] Morin-Brureau M, Lebrun A, Rousset MC, Fagni L, Bockaert J, de Bock F, Lerner-Natoli M. Epileptiform activity induces vascular remodeling and zonula occludens 1 downregulation in organotypic hippocampal cultures: role of VEGF signaling pathways. J Neurosci 2011; 31: 10677-10688
[11] Morin-Brureau M, Rigau V, Lerner-Natoli M. Why and how to target angiogenesis in focal epilepsies. Epilepsia 2012; 53 Suppl 6: 64-68
[12] Penfield; W, Jasper; HH, McNaughton; F. Epilepsy and the functional anatomy of the human brain. Churchill, 1954
[13] Haglund MM, Ojemann GA, Hochman DW. Optical imaging of epileptiform and functional activity in human cerebral cortex. Nature 1992; 358: 668-671
[14] Marques JP, Kober T, Krueger G, et al. MP2RAGE, a self bias-field corrected sequence for improved segmentation and T1-mapping at high field. Neuroimage 2010;49:1271-1281
[15] Feldman RE, Dyvorne HA, Delman BN, et al. 7T Imaging of patients with focal epilepsy who appear non-lesional in diagnostic 1.5T and 3T MRI scans: first results. Proceedings of the Annual Meeting of the International Society for Magnetic Resonance in Medicine Toronto, Ontario, Canada 2015:0755
Figures