3130
Detection of Focal Cortical Dysplasia via quantitative T1-mapping1Brain Imaging Center (BIC), Goethe University Frankfurt, Frankfurt am Main, Germany, 2Department of Neurology, University Hospital Frankfurt, Frankfurt am Main, Germany, 3Department of Neuroradiology, University Hospital Frankfurt, Frankfurt am Main, Germany, 4Epilepsy Center Hessen, University Hospital Marburg, Marburg, Germany
Synopsis
Focal cortical dysplasias (FCD) are characterized by an increased cortical thickness and blurred junctions between white (WM) and gray matter (GM). A method for improved FCD detection is proposed, which is only based on quantitative maps of T1 relaxation time. Masks of WM, GM and CSF are derived from the measured T1 values. The local cortical extent (CE) is calculated from the GM mask and the local smoothness (SM) of GM-WM junctions is derived from the T1 gradients. Synthetic double inversion recovery data sets are calculated from the T1 map and further enhanced in areas of increased CE and SM.
Introduction
Focal cortical dysplasias (FCD) belong to the most frequent cortical malformations, constituting subtle focal disorganization of the cerebral cortex. In particular, FCDs are a frequent cause of epilepsy in children and adolescents as well as in adults. In conventional MRI, FCDs may be characterized by focal cortical thickening, blurring of the junctions between gray (GM) and white (WM) matter, and - depending on the type of FCD - hyperintensity of subcortical WM on T2-weighted images1. Since these effects are rather subtle, the identification of FCDs on the basis of conventional MR images can be challenging. The purpose of this study was the exploitation of quantitative T1 maps for the improved detection of FCDs.Methods
Patients: Patients gave written informed consent before participation. 12 patients with epilepsy that were neuroradiologically suspected with FCD were included in the study. For each patient, T1 mapping and subsequent data analysis were performed as described below.
MR protocols: T1 mapping was performed on a 3T whole body scanner (body TX-coil, 8-channel phased-array head RX-coil), using the variable flip angle (VFA) technique2. Parameters were: FoV=256x224x160mm3, 1mm spatial resolution, TR/TE=16.4ms/6.7ms, FA1/FA2=4°/24°, duration 9:48min. B1 was mapped according to3. Quantitative T1 maps were calculated as described in the literature4.
FCD Detection: The method utilizes quantitative T1 data, only, and comprises five steps:
1. Segmentation: WM, GM and CSF masks are derived from local T1 values5. To identify small WM and CSF structures embedded in GM, the T1 gradient (G) is calculated and areas of marked local T1 maxima and minima are attributed to CSF and WM, respectively.
2. Calculation of the smoothness (SM) of WM-GM junctions: Junctions are subdivided into three layers. The T1 gradient G and its standard deviation std(G) are calculated across these layers and SM is given by SM~1/[G*std(G)].
3. Calculation of cortical extent (CE): For each pixel inside the GM mask, the distance (D) to the mask boundary is derived. Subsequently, twice the value of the local maximum of D is attributed to surrounding pixels within distances smaller than D, yielding the CE map.
4. Calculation of synthetic anatomies: A synthetic double inversion recovery (DIR) data set showing mainly GM structures is derived from the T1 map by using low-pass and high-pass Fermi filters with a maximum sensitivity at about T1=1600ms. Additionally, a synthetic MPRAGE data set is calculated6.
5. Enhancement of DIR data: The DIR data are enhanced on the basis of a parameter P (which may be CE or SM, both scaled from 0 to 1) according to: DIR(enhanced)=DIR*(1+k*P). Here, k=4 was chosen.
Results
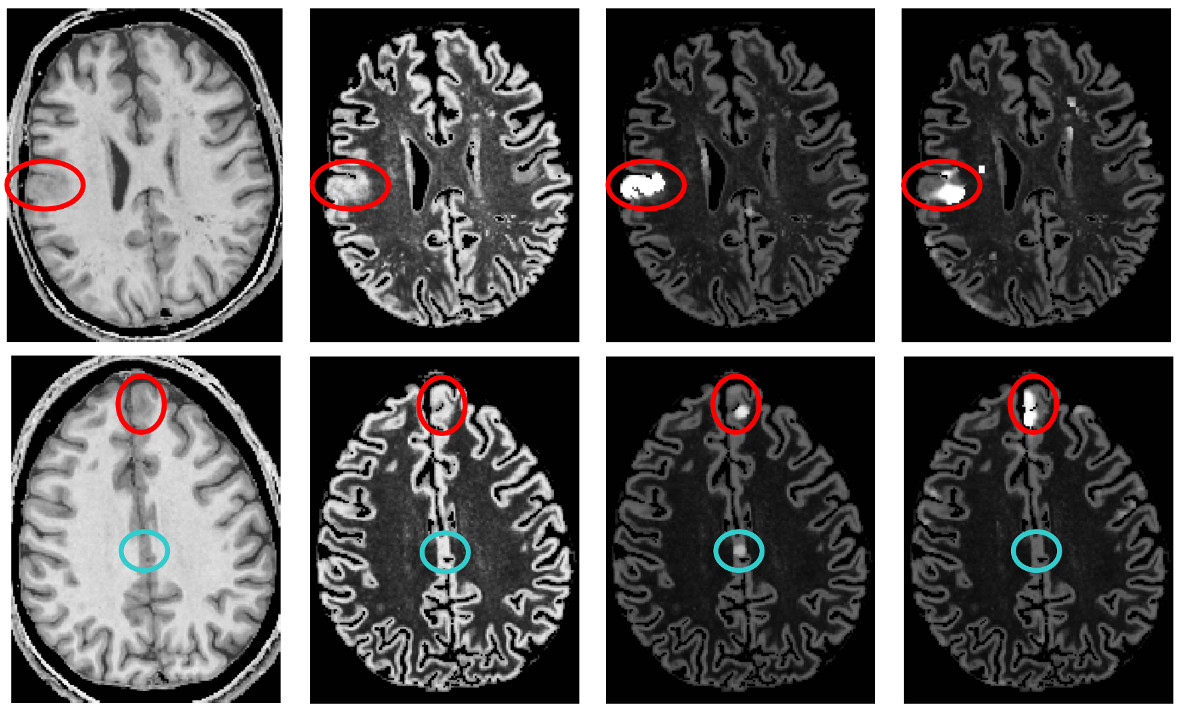
Figure 1 shows for two patients (rows) from left to right: synthetic MPRAGE, synthetic DIR, DIR enhanced via CE (CE-DIR), DIR enhanced via SM (SM-DIR). In both cases, an FCD which is already visible in the MPRAGE and the DIR data appears hyperintense in the enhanced DIR data sets (red circles). It should be noted that due to the enhancement method the location of the enhancement is slightly different for the CE-DIR and the SM-DIR. For one patient (bottom row), a false positive is visible in the CE-DIR (blue circle). This is due to partial voluming effects which prevented the segmentation algorithm from fully detecting embedded CSF which was thus misinterpreted as GM, yielding apparent cortical thickening.Discussion
The proposed method supports FCD detection. Still, it should be noted that the method may yield false positives: Firstly, due to partial voluming effects, CSF in the sulci may not be recognized correctly, yielding erroneously high CE values which appear hyperintense in the CE-enhanced DIR. Secondly, small structures with increased T1 extending into WM, such as perivascular spaces or the striatum, appear hyperintense in the SM-enhanced DIR. Therefore, due to the high sensitivity but relatively low specificity, the method is intended as a supporting tool for an experienced neuroradiologist, in addition to standard clinical MR images.Acknowledgements
This study was supported by the LOEWE-Program “CePTER-Center for Personalized Translational Epilepsy Research”References
1. Kini L.G. et al., Computational analysis in epilepsy neuroimaging: A survey of features and methods. NeuroImage: Clinical 2016; 11:515–529
2. Venkatesan R et al., Accurate determination of spin-density and T1 in the presence of RF-field inhomogeneities and flip-angle miscalibration. Magn.Reson.Med. 1998;40:592-602
3. Volz S et al., A fast B1-mapping method for the correction and normalization of magnetization transfer ratio maps at 3 T. NeuroImage 2010;49:3015-326
4. Preibisch C and Deichmann R: The influence of RF spoiling on the stability and accuracy of T1 mapping based on spoiled FLASH with varying flip angles Magn.Reson.Med. 2009;61:125-135
5. Volz S et al., Correction of Systematic Errors in Quantitative Proton Density Mapping. Magn.Reson.Med. 2012;68:74-85
6. Nöth U et al., Improved visibility of brain tumors in synthetic MP-RAGE anatomies with pure T1-weighting. NMR in Biomedicine 2015;28:818-830
Figures