3128
Morphology Analysis of Dilated Virchow Robin Spaces in Simple Febrile Seizure Children Between 12 and 48 Months Based on the Automated Segmentation1Department of Radiology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China, 2MR research china, GE health care, Beijing, China, 3Xi’an AccuRad Network and technology Co. Ltd., Xi’an, China, 4Department of Biomedical Engineering, School of Life Science and Technology, Xi’an, China
Synopsis
Febrile seizure (FS) has become a common problem in childhood and imposes acute effects on the brain. Currently dilated Virchow -Robin spaces (dVRs) has become hot point in research for the explanation the mechanism how its involving brain in inflammatory lesions. we conducted a quantitative method to assessment dVRs that visible onT2WI in simple FS. Our study aim is to describe an effective uses of automatic software method to recognize VRs and to get intergroup differences. Our result suggests that dVRs count, volume and head circumference are greater simple FS than in the control group.
Introduction
Febrile seizure (FS) has become a common challenges in childhood and imposes acute effects on the developing brain lesions. Neuroinflammatory mediators play an essential role in the mechanism of seizure1. VR spaces has an effective role in the inflammatory reaction in the brain. VRs alteration have become interesting part in the pathophysiology of the brain now days. Quantification of dVRs has been widely used in several pediatrics and neuroinflammatory lesions2. However, there have been few studies evaluating of dVRs in simple FS. Therefore, this study aims were to assess the quantification of dVRs visible on convention MRI and investigate their correlations with simple FS.MATERIALS AND METHODS:
This study included 70 simple FS children age range 12-48 months with clinical history of simple FS seizures, compared with 35 control groups of age matching who underwent MRI examination using 3T scanner (Signa HDxt, GE Healthcare, Milwaukee, Wisconsin, USA) with an 8-channel head coil. We acquired T2 weighted sequence (TR/TE, 4200ms/120 ms; matrix, 256*256; slice thickness, 2.5 mm; FOV, 240 mm) and T2 FLAIR sequence (TR/TE, 8600 ms/165 ms; matrix, 288*224; slice thickness, 5 mm; FOV, 240 mm). in our hospital between 2013 and 2017. The severity of dVRs was evaluated semi quantitatively and quantitatively in the region of white matter (WM) and basal ganglia (BG) using T2WI. Semiquantitative visual assessment, were rated 0 (none), 1. (1–10), 2. (11–20), 3. (21–40) and 4. (>40) per slice with maximum number in the region of BG and WM observed manually 3. Firstly, dVRs was fully automated segmented, axially T2WI were processed, the aid of the FMRIB software library (FSL, www.fmrib.ox.au.uk/fsl), eliminate masks of cortical gray matter, white matter, and CSF. Then after the images were shifted from FSL to Matlab (https://www.mathworks.com) for VRs quantification. Then Mann Whitney U test was used for comparison of the dVRs parameters between three groups. The bivariate Spearman’s rank was used to get the correlation between the severity of dVRs with time of seizure duration were compared inter groups.Results
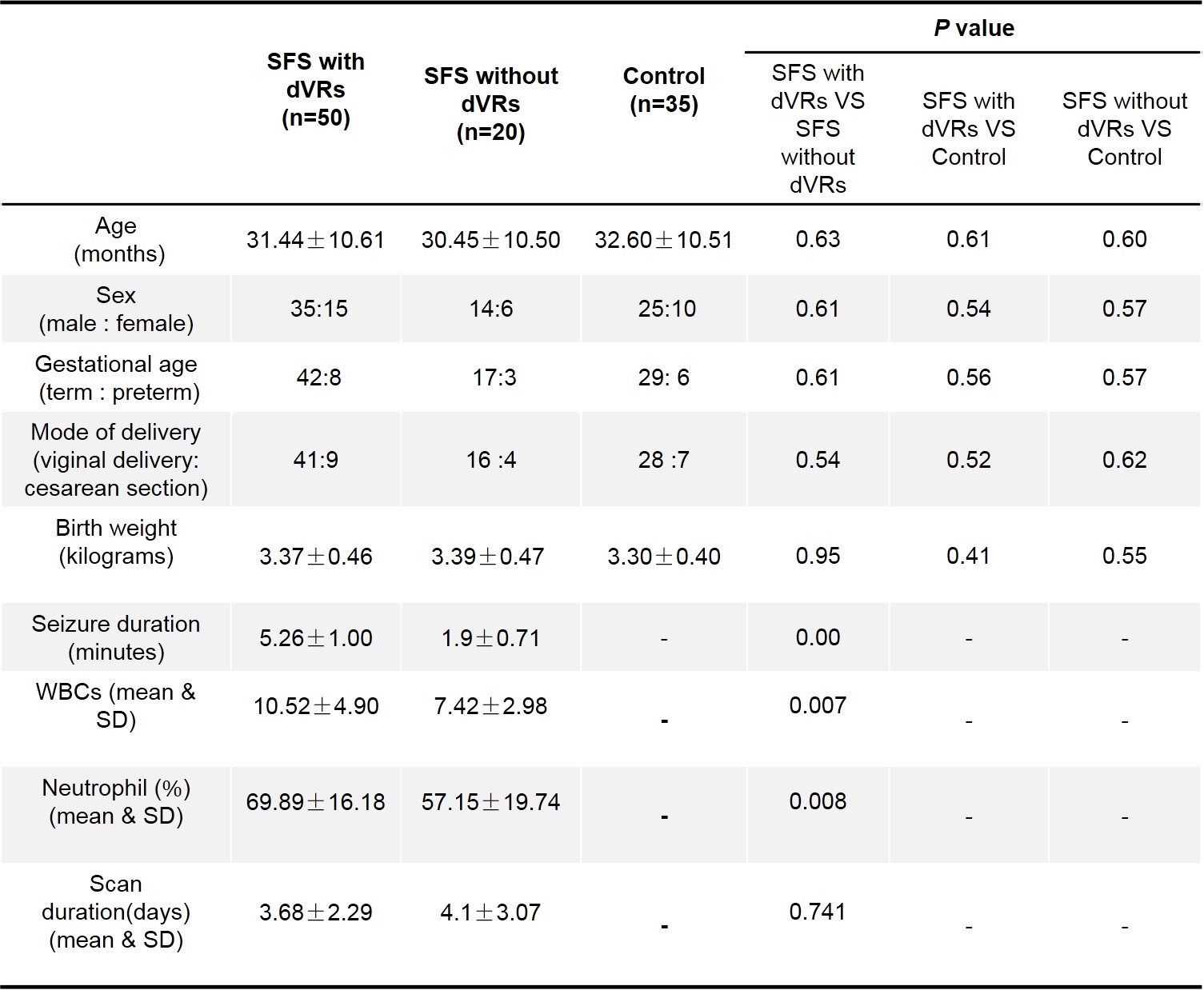
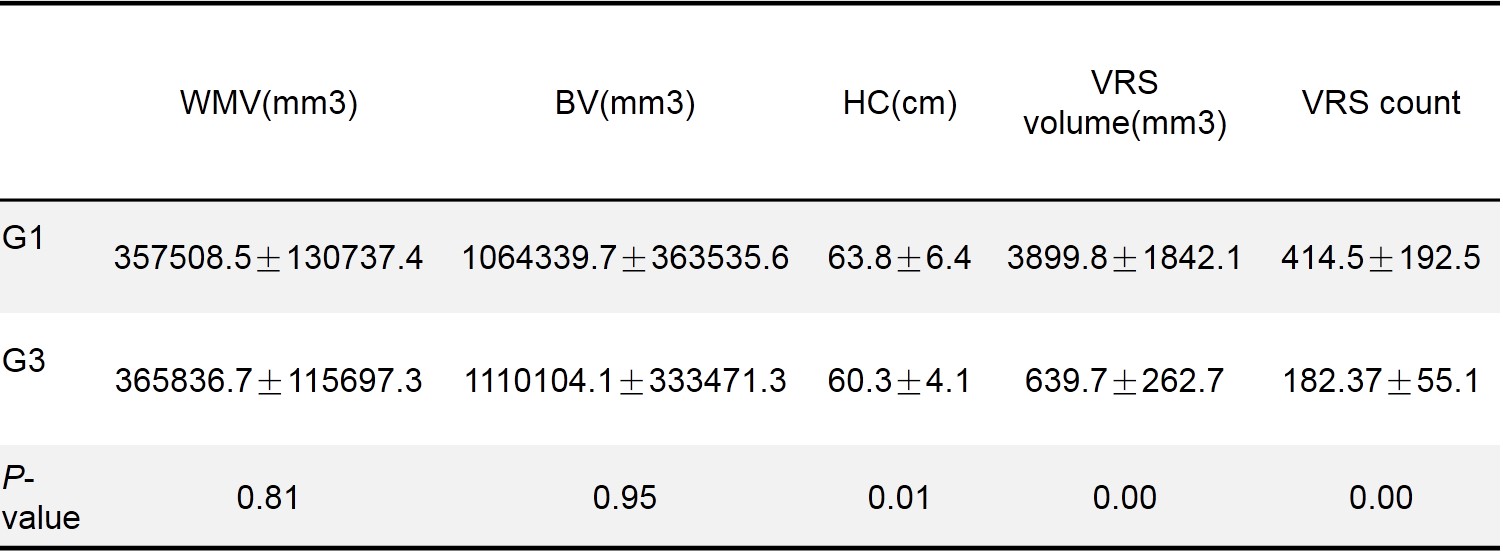
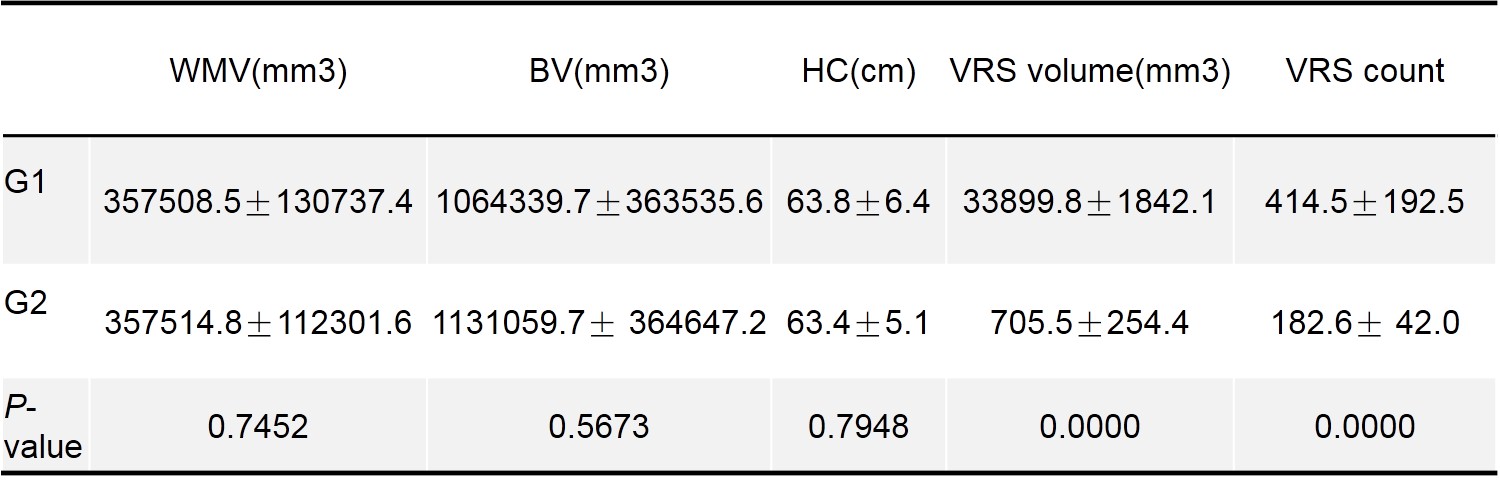
There was significant difference between simple FS patients with dVRs G1 and simple FS patients without dVRs G2 in seizure duration (Table 1), (P <0.001) and neutrophil, white blood count (WBCs), (P = 0.008), (P=0.007), respectively (Table1). Compared with G1, no significant difference in the time after controlling the seizure and scanning was found in G2 (P= 0.741) (Table1). Our semi quantitative methods finding showed excellent agreement which supporting our hypothesis. Inter-rater and intra-rater reliability of our visual rating score were excellent, Intraclass Correlation Coefficient (ICC) for simple FS patients were (ICC = 0.985, CI 0.9780.990) and (ICC = 0.850, CI 0.787- 0.895) respectively and for control group were (ICC =0.987, CI 0.981- 0.991) and (ICC = 0.969, CI 0.955- 0.979) respectively. VRs Segmentation findings there are significant of VRs volume and count for (G1), compared with (G2) and (G3) while, head circumference was only significant finding between (G1) and (G3) (table 2 and 3).Discussion
Based on study findings provide an evidence that dilatation of dVRs might be associated to seizure activities, there was a significant difference between the severity of dVRs in simple FS patients compared with simple FS without dVRs and control in the white matter region (p <0.00), (p <0.000) respectively. There was strong associated was founded between neuroinflammatory and neurodegerative disorders with the prevalence of dVRs in clinical practice4. The study strength in comparison to previous studies is based on the established pathophysiological correlation between simple FS seizure and dVRs. In our study we observed increased number of dVRs following long seizure duration (table 1). These observations indicating the active participation of dVRs in the immune response chain during simple FS with relatively long seizure. These findings are in consistence with other acute inflammatory biomarkers of seizure, established by histopathology studies 5 and serum immune mediators6. Both visual and automated method showed strong evidence in supporting our study hypothesis. However, there were higher numbers of dVRs counts in automated segmentation finding, suggesting that more dVRs can detect when using the quantification employed by automated software and may improve the accuracy of dVRS counting compared with visual methods. Reliability and reproducibility are essential are precise in quantification of dVRS.Conclusion
This study demonstrated that increased number of dVRS was more prominent in simple FS with long seizer duration. Full automatic segmentation is feasible to recognize all VR space in simple FS childrenAcknowledgements
The study was supported by the National Key Research and Development Program of China (2016YFC0100300), National Natural Science Foundation of China (No.81171317, 81471631, 81771810), the 2011 New Century Excellent Talent Support Plan of the Ministry of Education, China (NCET-11-0438), the Clinical Research Award of the First Affiliated Hospital of Xi’an Jiao Tong University (No. XJTU1AF-CRF-2015-004), the Fundamental Research Funds for the Central Universities (xjj2018265), the Fundamental Research Funds of the First Affiliated Hospital of Xi'an Jiaotong University (2017QN-09).References
1. Doubal, F. N., Maclullich, A. M. J., Ferguson, K. J., Dennis, M. S. & Wardlaw, J. M. Enlarged Perivascular Spaces on MRI Are a Feature of Cerebral Small Vessel Disease. Stroke 41, 450–454 (2010).
2. Wuerfel J, Haertle M, Waiczies H, et al. Perivascular spaces: MRI marker of inflammatory activity in the brain? Brain 2008; 131:2332–2340
3. Potter GM, Chappell FM, Morris Z, et al. Cerebral perivascular spaces visible on magnetic resonance imaging: development of a qualitative rating scale and its observer reliability[J]. Cerebrovasc Dis, 2015, 39 (3-4): 224-23
4. Ramirez J, Berezuk C, McNeely AA, et al. Imaging the perivascular space as a potential biomarker of neurovascular and neurodegenerative diseases. Cell Mol Neurobiol 2016;36:289–99.
5. Bakker EN, Bacskai BJ, Arbel-Ornath M, et al. Lymphatic clearance of the brain: perivascular, paravascular and significance for neurodegenerative diseases. Cell Mol Neurobiol 2016; 36:181–94.
6. Bechmann I, Priller J, Kovac A, et al. Immune surveillance of mouse brain perivascular spaces by blood-borne macrophages. Eur J Neurosci 2001;14:1651–8.
Figures