3116
High-quality FLAIR and diffusion imaging with presence of EEG nets1Department of Radiology, Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Boston, MA, United States, 2Philips, Eugene, OR, United States, 3Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 4Department of Radiology, Harvard Medical School, Boston, MA, United States, 5Department of Biomedical Engineering, Boston University, Boston, MA, United States
Synopsis
EEG nets are typically removed before MR imaging due to their negative effects on image quality, which is time-consuming and interrupts monitoring of brain activity. We tested whether the InkNet, a high-resistance polymer thick-film based EEG net, could improve images by reducing RF-shielding caused by copper leads. We imaged subjects with FLAIR and diffusion at 3 Tesla, wearing a conventional, copper-lead net, the InkNet, or no EEG net (NoNet). The InkNet induced less artifact than conventional nets, and produced similar image quality to the NoNet control. Results suggest that high-quality imaging can be achieved while wearing an EEG net.
INTRODUCTION:
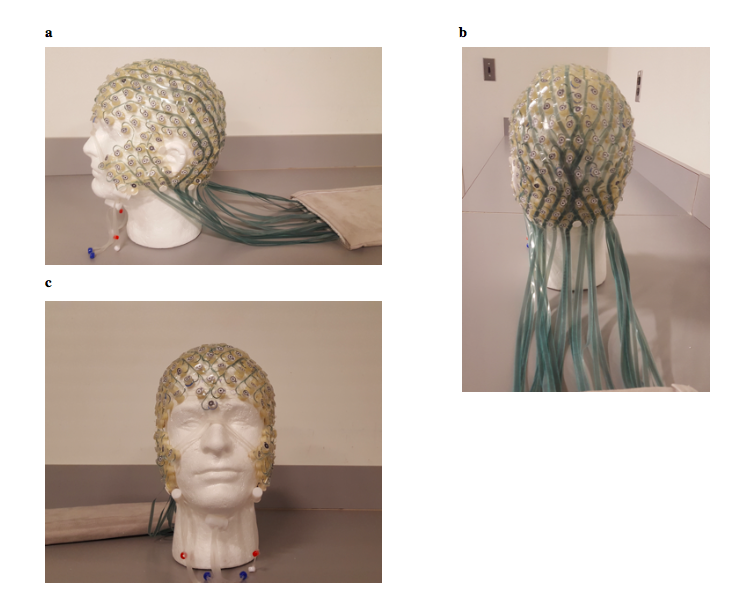
Patients undergoing EEG monitoring in the intensive care unit frequently need to undergo MR imaging. Typically, EEG nets must be removed prior to MR imaging, as they can severely impact image quality. This removal and re-application process is time-consuming and costly, and results in long periods of time where the EEG cannot be monitored, potentially impacting patient care. We investigated whether a new, 256-channel, high-resistance polymer thick film-based EEG net - the InkNet1 (Fig. 1) -, could allow high-quality clinical images to be acquired without the need to remove the EEG net. We tested how the InkNet impacted FLAIR and diffusion image quality and compared it to a standard 256-channel EEG net with copper leads (‘CuNet’) and a control condition with no net (‘NoNet’) at 3 Tesla.METHODS:
Two subjects gave informed consent and were scanned on a 3T Siemens Skyra scanner with a 32 channel head coil array. Each subject was scanned in three conditions: a control with no EEG net (NoNet), the CuNet – a commercial copper-lead net (HCGSN-MR, Philips, Eugene, OR), and the prototype InkNet. Each condition followed the same imaging protocol. In each condition, we acquired a 0.9 mm isotropic resolution single-shot T1 MPRAGE. FLAIR images were acquired with 0.9 mm isotropic resolution with 192 slices with whole-brain coverage (TR=5000 ms, TE=387 ms, FOV=230 mm, TI=1800 ms). The diffusion images were acquired with 25 interleaved slices with whole-brain coverage (TR=3700 ms, TE=92.0 ms, FOV=220 mm, Voxel size=1.7x1.7x4.0 mm). B1 maps were acquired with 16 slices with whole brain coverage (TR=11380.0 ms, TE=2.06 ms, FOV=208 mm, Voxel size=1.6x1.6x4.0 mm).
A radiologist was asked to analyze for the presence of artifact, the overall image quality, and the clinical usability, on a scale of 1 (best) to 5 (worst). The image was processed to exclude all signal outside the brain and skull, by manually masking any signal so that the EEG net was not present on the image, allowing an assessment of image quality while blinded to experimental condition.
We manually identified the regions of the scans where the CuNet artifact was present and compared these regions to our NoNet control. The B1 maps were processed and registered, and an ROI corresponding to the artifact region in the CuNet condition was segmented. This ROI was then mapped onto the InkNet and NoNet conditions. The flip angle for each voxel within this ROI was reported.
RESULTS:
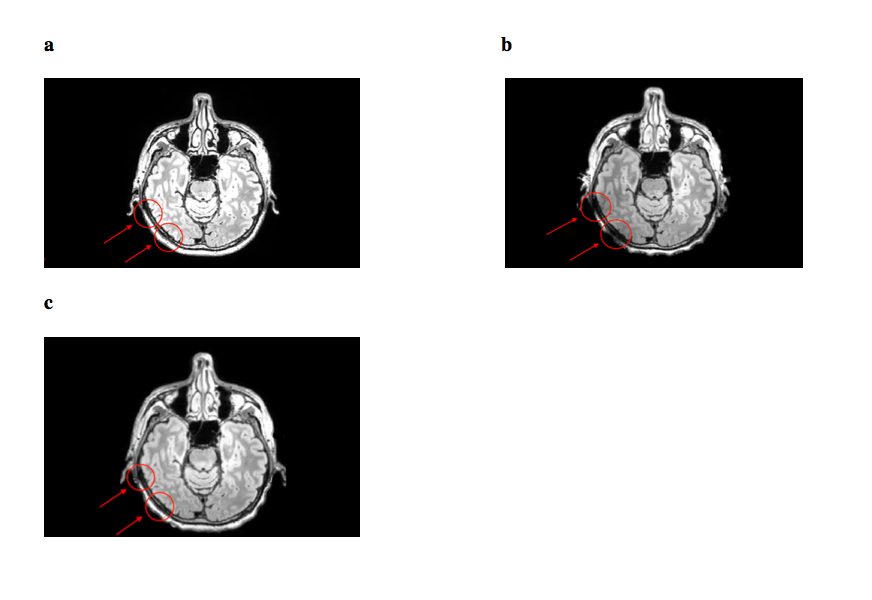
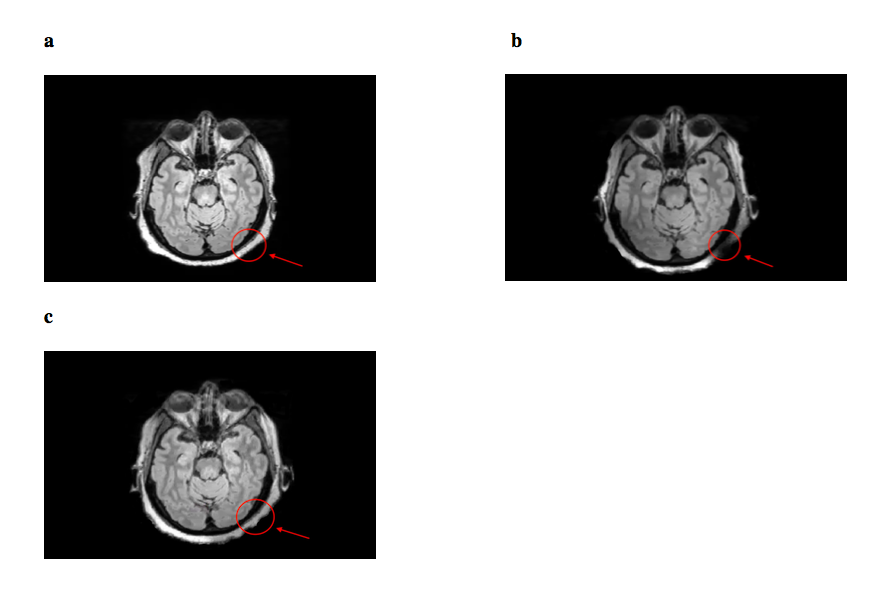
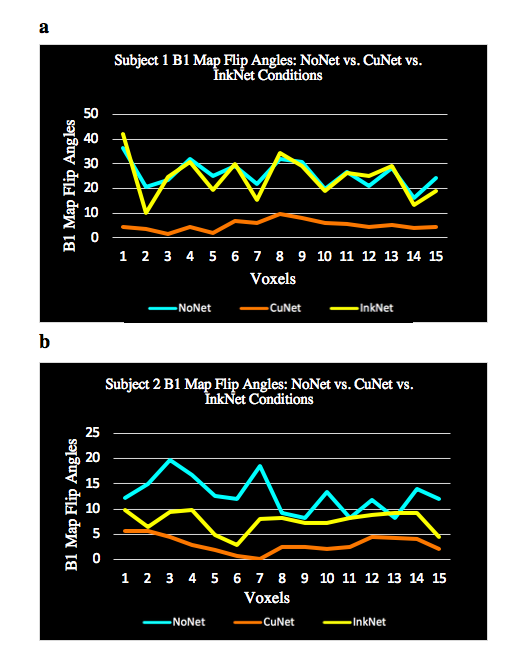
Visual inspection of the images identified clear artifacts induced in the images acquired with the CuNet (Fig. 2, 3). We calculated the flip angle for both subjects in the ROI where the artifact was most severe, and found consistently decreased values in the CuNet condition. For subject 1, the mean flip angle was 25.8° (NoNet), 24.5° (InkNet) and 5.2° (CuNet). For subject 2, the mean flip angles were 12.8° (NoNet), 7.6° (InkNet), 3.0° (CuNet). The values in individual voxels demonstrate that the B1 field maps were consistent in the InkNet and NoNet conditions, and much lower in the CuNet condition (Fig. 4), suggesting that the InkNet avoids inhomogeneity that can impact FLAIR and diffusion image quality.
To determine the clinical impact of these artifacts, a radiologist rated the presence of artifact and image quality, while blinded to condition (1 = no artifact present, high image quality; 5 = severe artifact present, low image quality). For both subjects, the FLAIR images were rated as: 1 (NoNet), 1 (InkNet), 2 (CuNet). For both subjects, the diffusion images had ratings of: 1 (NoNet), 1.5 (InkNet), and 2 (CuNet).
DISCUSSION:
Our data suggest that using the InkNet can allow similar quality FLAIR and diffusion sequences as seen without an EEG net at 3 Tesla. Comparison of the B1 maps, the intensity difference of the images, and the qualitative evaluation by a radiologist all suggest that there are better signal quality and less artifact with the 256-channel InkNet in comparison to the standard 256-channel CuNet.CONCLUSION:
Our data suggest that using the high-resistance-lead InkNet will allow researchers and clinicians to be able to use FLAIR and diffusion sequences with MR-EEG without compromising image integrity. Integration of the InkNet would also allow for researchers to move from EEG/fMRI to FLAIR or diffusion sequences without having to remove the EEG net. For clinicians, the use of the InkNet could allow them to save time and reduce spending due to not having to reapply EEG nets. Future work could examine whether the InkNet allows other sequences to be run simultaneously while still maintaining high-quality clinical images.Acknowledgements
This work was funded by NIH/NINDS grant R44NS071988 and by NIH grant K99-MH111748. This work was also supported in part by the MGH/HST Athinoula A. Martinos Center for Biomedical Imaging.References
1) Poulsen, C., Wakeman, D. G., Atefi, S. R., Luu, P., Konyn, A., & Bonmassar, G. (2016). Polymer thick film technology for improved simultaneous dEEG/MRI recording: Safety and MRI data quality. Magnetic resonance in medicine, 77(2), 895-903.Figures