3114
Improved imaging method for comprehensive diagnosis of cervical artery disssection1Jilin University First Hospital, Changchun, China, 2Philips healthcare, Changchun, China
Synopsis
Cervical artery dissection (CAD) is a significant cause of ischemic stroke in young adults. As a result, the early and accurate diagnosis of CAD is helpful for appropriate treatment decision-making to prevent stroke. Traditional imaging methods, such as CTA, MRA or DSA are difficult to differentiate CAD from other mimics because of similar luminal findings1,2. 3D T1-weighted black blood sequence would demonstrate the abnormality of vessel wall and could potentially provide diagnosis information for vasculopathy patients. This study aims at introducing a 3D black-blood sequence’s application in the diagnosis of CAD, as well as atypical artery dissection.
Purpose
Previous studies have demonstrated the use of the three-dimensional (3D) T1-weighted sequence of volumetric isotropic turbo spin echo acquisition (VISTA) at 1.5 Tesla to diagnose cervical artery dissection (CAD)3,4. This study aimed to investigate the value of 3D T1 VISTA at 3.0 Tesla in diagnosing CAD and discuss its limitations.Material and Methods
Patients clinically suspected as having CAD within 1 month of onset were included in this study. All patients received 3D T1 VISTA examination at 3.0 Tesla MRI scanner(Philips Healthcare, Ingenia, Best, the Netherlands) and at least one examination of magnetic resonance angiography (MRA), computed tomography angiography (CTA) or digital subtraction angiography (DSA). For atypical CAD,we chose color-mode ultrasound to find avulsion of the inner diaphragm. The analysis of all imaging results was performed by two experienced neuro-radiologists who were blinded of the patient information and final diagnosis. For T1 VISTA, the diagnosis of CAD was based on the presence of intramural hematoma, intimal flap, double lumen, and aneurysmal dilation. The final diagnosis of dissection was based on clinical history, physical examination, and all imaging tests. SPSS V.19.0 (IBM, West Grove, Pennsylvania, USA) was used for the analysis. As no gold standard for the diagnosis of CAD was available, the final diagnosis results were chosen to be reference standards to calculate the sensitivity and specificity (including the corresponding 95% CI) for 3D T1 VISTA. The interobserver agreement for 3D T1 VISTA was examined by using theκ-coefficient of agreement of agreement. The Fisher’s exact test was used to count data. The level of statistical significance was set at p<0.05.Results
A total of 46 patients were included in this study. The final diagnosis of CAD was made for 21 patients. Diagnosis of dissection was made for 20 of the 21 patients after assessing T1 VISTA. The sensitivity and specificity for T1 VISTA were 95.2%(95% CI, 76.2% to 99.9%) and 100%(95% CI, 86.3%to 100%), respectively. The agreement between the two researchers for T1 VISTA for diagnosis of CAD was very good (k=0.91). All patients without acute artery occlusion had a definite conclusion with or without dissection by T1 VISTA (n = 29). However, the possibility of dissection could not be excluded for 6 of 17 patients with acute artery occlusion using T1 VISTA (P = 0.001). These patients underwent artery dissection using color-mode ultrasound demonstrating denudated endometrium tissue, flow detection of occluded distal segment artery, and a half-year follow-up of expansion and opening of the dissection artery.Discussions
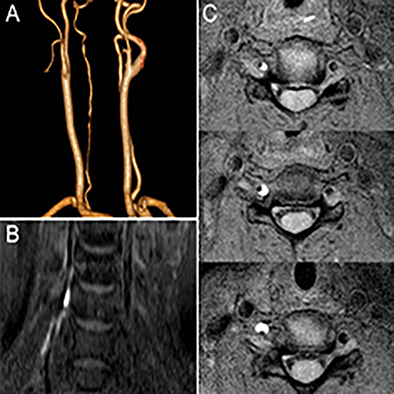
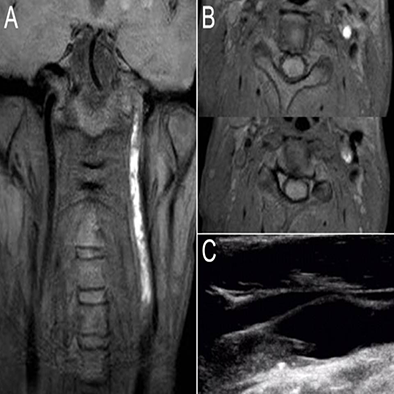
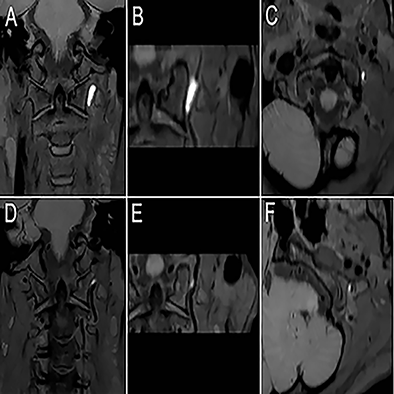
A 3D T1-weighted black-blood sequence with black-blood techniques is able to suppress the flowing blood and surrounding vessels’ signal in the lumen5. The blood flow signal in lumen is low, while that in interstitial hematoma is relatively high. Such signal difference is useful in detecting interstitial hematoma (Fig.1). 3D T1 VISTA at 3.0 Tesla was useful in the diagnosis of acute CAD in this study. However, for some patients with total occlusion of the artery without typical imaging features of dissection, the unequivocal distinction between intramural haematoma and intraluminal thrombus may not be possible by T1 VISTA alone. Color-mode ultrasound(Fig.2) and follow-up(Fig.3) are good options. The innovative multimodality imaging method together with consecutive follow-up provides more comprehensive information on atypical patients. For instance, the color-mode ultrasound can provide a perfect demonstration of avulsion of the inner diaphragm and the flow of distal segment led by artery dissection. The CAD is a dynamic process, 55~78% patients in this study showed partial or complete vascular recanalization6. Accordingly, the follow-up study of 3D VISTA sequence provided a good diagnosis for those patients without obvious imaging features with prior artery occlusion.Conclusion
3D T1 VISTA at 3.0 Tesla was useful in the diagnosis of acute CAD in most of the patients. However, for some patients with total occlusion of the artery without typical imaging features of dissection, the unequivocal distinction between intramural haematoma and intraluminal thrombus may not be possible by T1 VISTA alone. A multimodality imaging method and follow-up study can serve as a good compensation for the imaging diagnosis of these patients.Acknowledgements
No acknowledgement found.References
1.Biller J, Sacco RL, Albuquerque FC, et al. Cervical arterial dissections and association with cervical manipulative therapy: A statement for healthcare professionals from the american heart association/american stroke association[J]. Stroke; a journal of cerebral circulation. 2014.45:3155-317
2.Blum CA, Yaghi S. Cervical artery dissection: A review of the epidemiology, pathophysiology, treatment, and outcome[J]. Archives of neuroscience. 2015.2
3.Ortiz J, Ruland S. Cervicocerebral artery dissection[J]. Current opinion in cardiology. 2015.30:603-610
4.Mandell DM, Mossa-Basha M, Qiao Y, et al. Intracranial vessel wall mri: Principles and expert consensus recommendations of the american society of neuroradiology[J]. AJNR. American journal of neuroradiology. 2016
5.Bejot Y, Daubail B, Debette S, et al. Incidence and outcome of cerebrovascular events related to cervical artery dissection: The dijon stroke registry[J]. International journal of stroke : official journal of the International Stroke Society. 2014.9:879-882
6.Choi YJ, Jung SC, Lee DH. Vessel wall imaging of the intracranial and cervical carotid arteries[J]. Journal of stroke. 2015.17:238-255
Figures