3113
3D printed, patient-specific vascular models for 4D flow MRI: production workflow and imaging aneurysm treatment1Neuroradiology and Radiology, Section Biomedical Imaging, Molecular Imaging North Competence Center (MOIN CC), Department of Radiology and Neuroradiology, University Medical Center Schleswig-Holstein (UKSH), Kiel University, Kiel, Germany, 2Neuroradiology and Radiology, Department of Radiology and Neuroradiology, University Medical Center Schleswig-Holstein (UKSH), Kiel University, Kiel, Germany
Synopsis
Patient-specific models of the human vessels could be used for the different purposes varying from the visualization of a vasculature to examination of a strategy of the endovascular treatment.
Current work represents a step by step workflow of the production of vascular models: optimisation of the geometry of the digital model, design of the connectors, wall thickness of the model etc. The flow in the models was compared with in vivo flow data of the patient.
The influence of different flow diverter stents on the flow in the model with an aneurysm was evaluated with MRI (TOF and 4D Flow).
Introduction:
Patient-specific vascular flow models are used e.g. for training, practicing, identifying optimal - or testing new treatments. 4D flow MRI allows measuring repetitive flow patterns in vivo and in vitro.
In this work, we present a workflow to produce patient-derived, vascular models using 3D printing technology. We tested these models by imaging the flow in an aneurysm model with and without three different flow-diverter stents.
Methods:
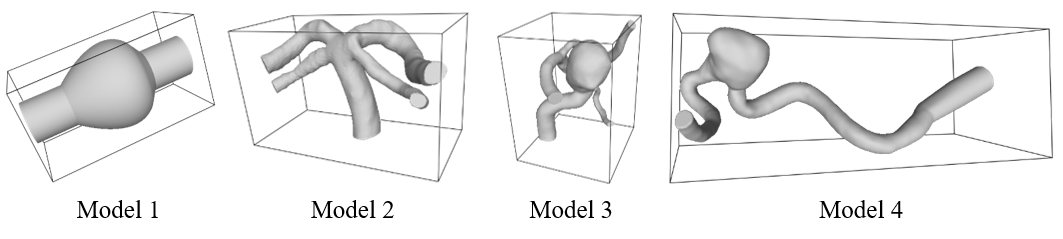
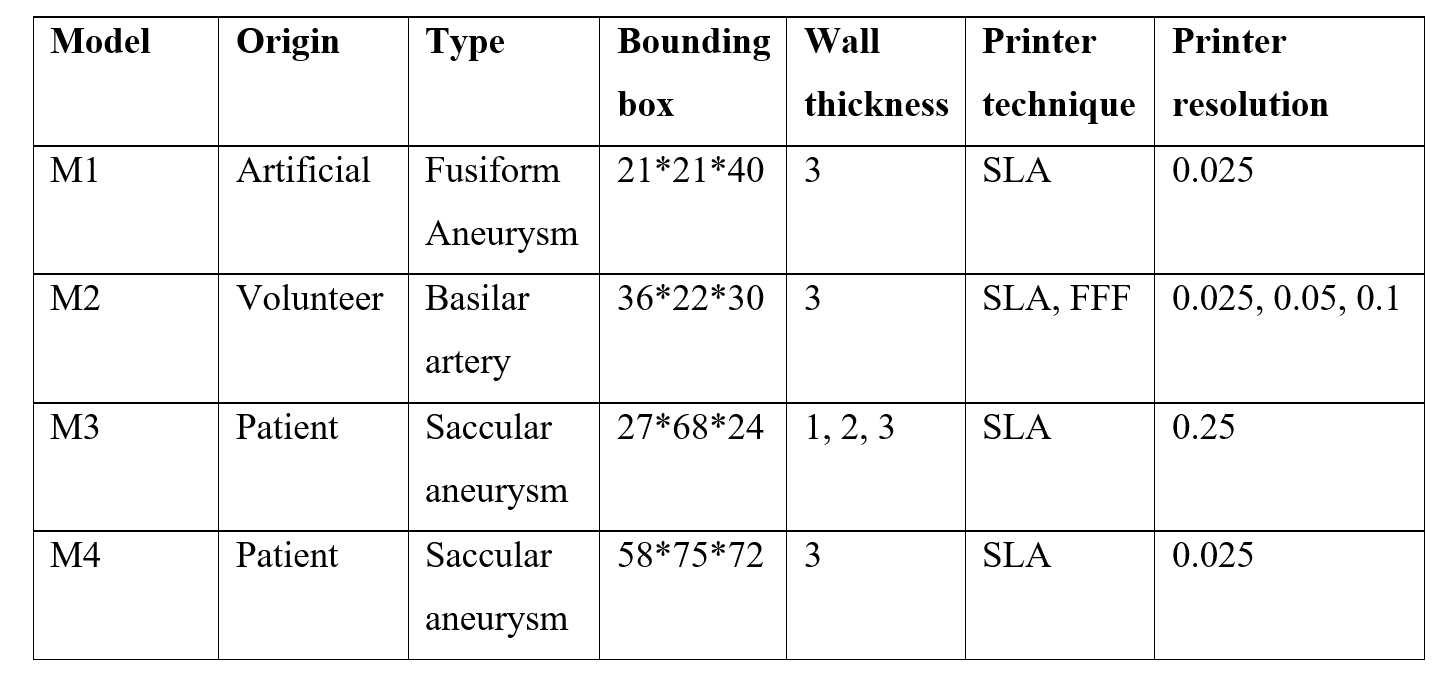
Production workflow: a digital model of the patient's vasculature was created as follows: 1. Generation of a digital vessel from medical images (3D rotational angiography and MRI), 2. Model optimization (closing holes, separating vessel etc.), 3. Adding connectors and 4. Printing with 3D stereolithography (Form 2, Formlabs) (Autodesk fusion, Meshmixer). Four different types of models were produced (M1-4, Fig. 1). M1 was printed with different connectors, M2 with different in-plane resolution (25, 50, 100mm), M3 with three different wall strengths (1, 2, 3mm) and M4 was used for the stent evaluation test (13 models total, Figure 1, Table 1). The accuracy of model M3 was compared to in vivo patient data (f, 52y) by 4D flow MRI (gradient echo (GRE), 3D, TE 3.4ms, TR 5.2 ms, flip angle (FA) 10°, bandwidth (BW) 1352 Hz, prospective ECG gating).
Treatment comparison: time-of-flight (TOF) (GRE, 3D, TE 3.5ms, TR 25ms, FA 20°, BW 217 Hz) and 4D-flow MRI (GRE, 3D, TE 5.1ms, TR 12ms, FA 8°, BW 588 Hz, prospective ECG gating, and processing with GTflow, Gyrotools) was acquired at 3 T (Philips Achieva) before and after the stents (P64, Phenox; Derivo, Acandis; Silk, Balt Extrusion) were placed in M4 by an experienced neuroradiologist. Hemodynamic parameters (velocity, pressure, vorticity) were calculated based on 4D flow MRI and evaluated in the entire volume, aneurysm sac, and healthy vessel.
A glycerin-water mixture was pumped through M4 using a pulsatile flow pattern similar to humans (2 and 5 ml/s mean flow rate, CompuFlow 1000, Schelley Medical).
Results:
Production workflow: in total, 13 vascular models were successfully produced without apparent failures (Figure 1).
Neither printing resolution nor wall thickness had an apparent effect on the flow patterns and MRI. Considering stability and transparency of the model, 2 mm wall thickness was chosen for the further investigations.
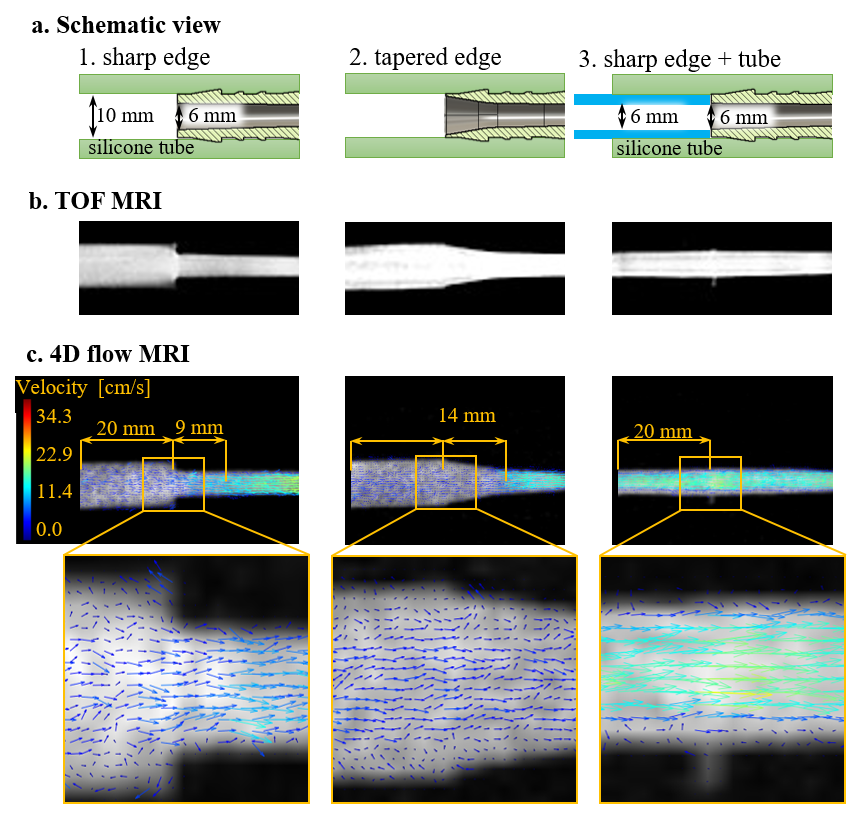
The connections exhibited a strong impact on the flow patterns (Figure 2). Here, type 3 provided the most homogenous flow.
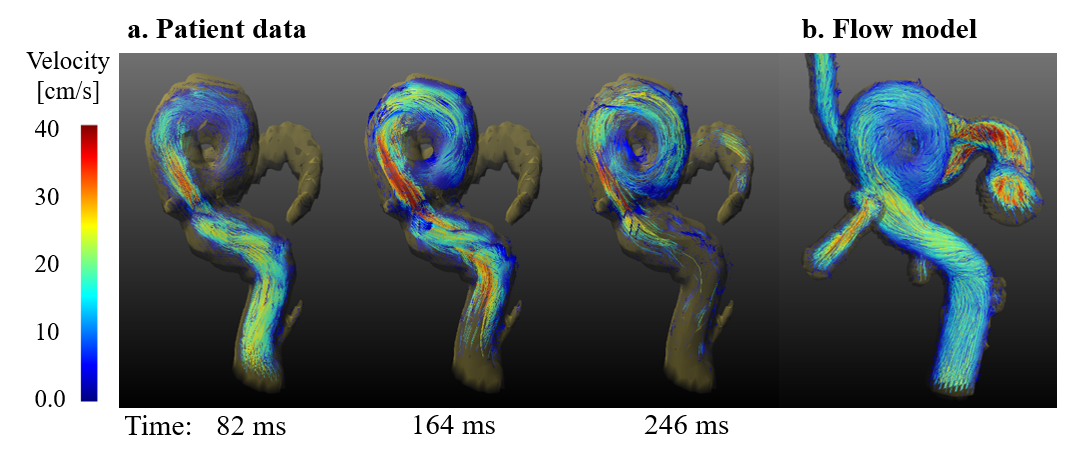
The flow in M3 was compared to in vivo data (Figure 3), and all basic features were reproduced. However, it should be noted that the model was supplied with constant flow only.
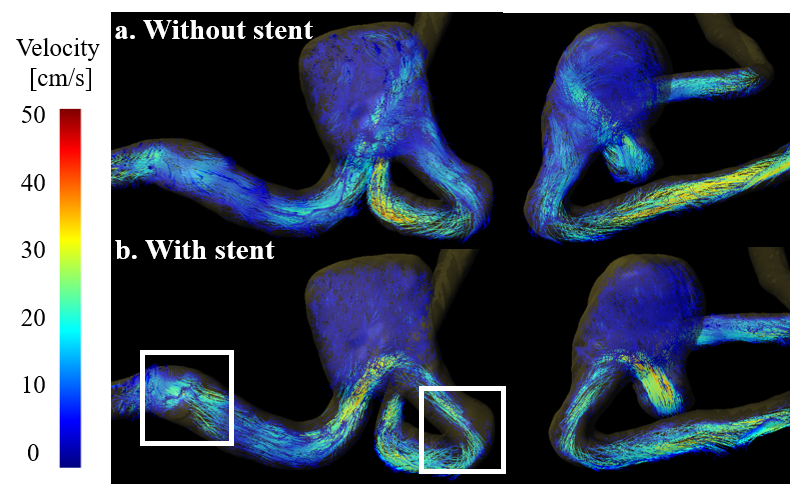
Treatment comparison: both TOF and 4D flow MRI exhibited a strongly reduced flow into an aneurysm after stent placement (Figure 3). However, some artifacts were apparent, likely attributed to field distortions caused by the stent materials. No significant differences in SNR of the TOF were observed for different stents. The hemodynamic parameters were different for each stent, especially in the aneurysm sac.
Discussion:
The presented workflow is a comparably simple and fast method to obtain patient-derived models of the vasculature. Most issues arise in producing the digital model – here, the user has to make subjective choices e.g. on which vessels to keep or crop.
The current material is rigid, - for a more realistic model, a more flexible material is recommended (some available and under investigation).
The connectors have a strong effect on the flow. This result emphasizes the importance of choosing the right one for reliable results. Note, though, that only repetitive flow patterns are depicted by 4D flow MRI, turbulent flows will likely cancel.
The comparison of flow between models and patients is promising but requires further investigation with an increased number of patients and using the patient-specific pulsatile flow pattern.
The developed models were well suited to assess the effects of stent treatment on the flow. The effect was strong and obvious – a reliable, more quantitative analysis, however, was found to be difficult. Many hemodynamic parameters were readily provided by the software and calculated for different segments. The results, however, were mixed and should not be trusted blindly. Reason for this likely include the fitting algorithms of the processing software, the fact that 4D flow measures only repetitive flow patterns and artifacts from the stents.
Conclusion:
A concise protocol for the fabrication of patient-specific models was successfully developed. In the first assumption - with constant flow, models are able to catch the patient flow pattern.
In a first application, the models were found to be well suited to investigate the effect of stents on the flow at an aneurysm. Qualitatively, all stents investigated had a similar diversion effect. A more quantitative analysis, metal artifacts, properties of 4D flow and reproducibility have to be investigated.
Acknowledgements
This work was funded by the German Research Foundation (DFG) as part as of the Research Training Group “Materials4Brain” (GRK2154; P2)References
No reference found.Figures