3106
Online brain fMRI using a novel magnetic resonance compatible hand induced robotic device provides accurate monitoring and can be used in rehabilitation1NMR Surgical Laboratory, Department of Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States, 2Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, United States, 3Neuroscience Center, Departments of Neurology and Neurosurgery, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, United States
Synopsis
Using a hand motor task, we investigated brain activation after chronic stroke by combining fMRI at 3T with a novel MR-compatible hand-induced, robotic device (MR_CHIROD). Patients trained at home using a gel ball; serial neuroimaging was performed before, during, upon completion of training, and after a non-training period, to assess permanence of effects. Training significantly increased the number of activated voxels in the cortex as a function of effort level, suggesting functional cortical plasticity in chronic stroke. The result’s persistence indicates permanence of rehabilitation, which is remarkable given that training is generally effective during a narrow window after stroke.
Introduction
Brain
imaging studies in chronic stroke patients have shown evidence for plastic
changes co-localization of areas showing structural and functional plasticity
after a stroke1. Training-induced reorganization of the motor
system has been consistently reported, leading to improvements in function
commonly seen over weeks, months, sometimes years after stroke2,3. Robot-assisted therapy has been shown to
result in significant gains in motor coordination and muscle strength of the
exercised shoulder and elbow, sustained in a three-year period following
discharge from the hospital4. Here, we present results combining motor fMRI
with a novel MR-compatible hand-induced robotic device (MR_CHIROD)5-8 to monitor rehabilitation after chronic stroke.Materials and Methods
Five male patients withMCA stroke ≥ 6 months prior and underwent serial MR evaluation before training, and at 4 wks, 8 wks and 12 wks after baseline. Home training consisted of squeezing an exercise ball with the paretic hand at 75% of max strength
for 1 hr/dy, 3 dys/wk. fMRI was
performed using GRAPPA gradient-echo EPI (TR/TE=3000ms/30ms, 1.56 mm×1.56 mm×3 mm) on a Siemens Tim Trio (3T). T1-MPRAGE and FLAIR
served as reference. A block design paradigm was used. During the action period,
subjects squeezed the MR_CHIROD and released continuously. Squeezing rate was
guided by a visual ‘metronome’ cue circle
oscillating radially at 0.5 Hz. A fixation cross was
projected during rest. Each volunteer performed the paradigm at 45%, 60%,
and 75% of their max grip strength and could fully squeeze the device at
all levels. Images were
normalized to MNI152 space and smoothed with a 4×(voxel dimension) Gaussian kernel. Significant voxels were P<0.05, corrected. Clusters of
statistically significant voxels were further selected for BOLD ≥ 2.0% 9. While the numerical value of
2.0% is in itself arbitrary, only cortical motor areas are consistently
activated at such BOLD values. The 2.0% threshold thus served as a filter,
selecting regions of interest without enforcing their boundaries a priori. Number counts of activated
voxels were averaged across subjects. Comparisons between effort levels (B-A,
C-A, Fig. 2) were done using t-test (two-tailed; normality of variances: P = 0.94, Shapiro-Wilks); P<0.05 was considered significant.Results
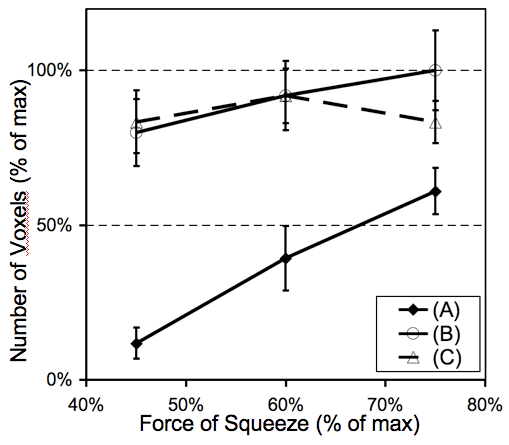
Increased force of squeezing resulted in increased activation in the SMC and recruitment of other cortical areas, especially the SMA (Fig. 1; and Fig. 2) and areas in the cerebellum. Fig. 2 shows that at 3 performance levels (45%, 60%, and 75% of max effort ) and at 3 time points (halfway through training, curve [A], at the end of training [B], and follow-up after training [C]) significant changes in the no. of activated voxels were observed. During the training period the no. of activated voxels increased with force of squeezing; at the end of the 1st training period the curve of activated voxels vrs force started from the final level achieved in the previous assessment and increased further from that point; and, 4 wks later the fMRI data indicated persistence of effects: changes that occurred during training were sustained after training (curve C). At 45% level, A (mean number of activated voxels ±SD, 35 ±15) differed from B (236 ±32), P= 0.0022, and from C (246 ±30), P= 0.0016. At 60% level, A (116 ±31) differed significantly from B (271 ±33), P< 0.05, and from C (271 ±26), P< 0.05. At 75% level A (180 ±22) differed significantly from B (295 ±38), P< 0.05, and from C (246 ±20 voxels) P< 0.05. At no effort level did the no. of activated voxels in C significantly differ from that at B.Discussion
In chronic stroke patients, increased squeezing force results in increased contralateral SMC and SMA activation, previously demonstrated in controls9,10. We suggest that training-induced functional cortical plasticity persists even in chronic stroke patients supported by previous reports11,12. Thus, rehabilitation of stroke patients can be induced by motor training, resulting in functional cortical plasticity. We suggest that online brain fMRI using novel hand devices provides accurate monitoring and can be used in rehabilitation.Acknowledgements
NIH/NINDS 1 R01 NS105875 01A1References
1. Schaechter, J.D., et al., Structural and functional plasticity in the somatosensory cortex of chronic stroke patients. Brain, 2006.
2. Nelles, G., Cortical reorganization--effects of intensive therapy. Restor Neurol Neurosci, 2004. 22(3-5): p. 239-44.
3. Ward, N.S., Future perspectives in functional neuroimaging in stroke recovery. Eura Medicophys, 2007. 43(2): p. 285-94.
4. Volpe, B.T., et al., Robot training enhanced motor outcome in patients with stroke maintained over 3 years. Neurology, 1999. 53(8): p. 1874-6.
5. Khanicheh, A., et al., MR Compatible ERF-Based Robotic Device for Hand Rehabilitation After Stroke. Proc. Intl. Soc. Mag. Reson. Med., 2005. 13: p. 1110.
6. Tzika, A.A., et al., Novel rehabilitation hand robots and fMRI in Stroke [Abstract]. European Radiology, Supplement1, 2006. 16: p. 183.
7. Khanicheh, A., et al., fMRI-compatible rehabilitation hand device. J Neuroengineering Rehabil, 2006. 3: p. 24.
8. Khanicheh A, et al., Magnetic Resonance Compatible Smart Hand Rehabilitation Device for Brain Imaging. IEEE Neural Systems and Rehabilitation Engineering, accepted.
9. Cramer, S.C., et al., Motor cortex activation is related to force of squeezing. Hum Brain Mapp, 2002. 16(4): p. 197-205.
10. Mintzopoulos, D., et al., On-line brain mapping using fMRI and a Magnetic Resonance Compatible Hand-Induced Robotic Device (MR_CHIROD). Proc. Intl. Soc. Mag. Reson. Med., 2007. 15: p. 3330.
11. Johansen-Berg, H., et al., Correlation between motor improvements and altered fMRI activity after rehabilitative therapy. Brain, 2002. 125(Pt 12): p. 2731-42.
12. Fasoli, S.E., et al., Robotic therapy for chronic motor impairments after stroke: Follow-up results. Arch Phys Med Rehabil, 2004. 85(7): p. 1106-11.
Figures