3104
Cerebral venous thrombus staging in a single magnetic resonance (MR) scan: A dual-contrast approach1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Philips Research North America, Cambridge, China, 3Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
This study proposed a dual-contrast Volumetric Isotropic Turbo spin echo Acquisition (dVISTA) sequence that allows both T1 and T2 cerebral venous thrombus imaging. In-vivo experiments indicated that dVISTA provide adequate image contrast as conventional T1/T2 imaging, and the clinical feasibility of this technique was further validated by CVT patients’ scan. By assembling flow-suppression, T1/T2 contrast in one 6-min whole brain scan, dVISTA has the potential to detect and differentiate thrombus in clinical routine.
INTRODUCTION
Cerebral venous thrombosis (CVT) is an uncommon and life-threatening condition, which requires early diagnosis1,2. Recent studies reported that T1-weighted black-blood magnetic resonance (MR) imaging can achieve directly detection of CVT3. However, given that both hyperacute (days) and chronic (> 1 month) thrombosis exhibit isointense signal in T1 MR images4, there is a potential pitfall in differentiating stages of CVT, thus requiring a multi-contrast MR imaging technique to address this limitation. In this study, we hypothesize that CVT can be accurately staged by combining T1 and T2 contrast in one scan, and propose a dual-contrast Volumetric Isotropic Turbo spin echo Acquisition (dVISTA) sequence that allows both T1 and T2 CVT imaging.METHODS
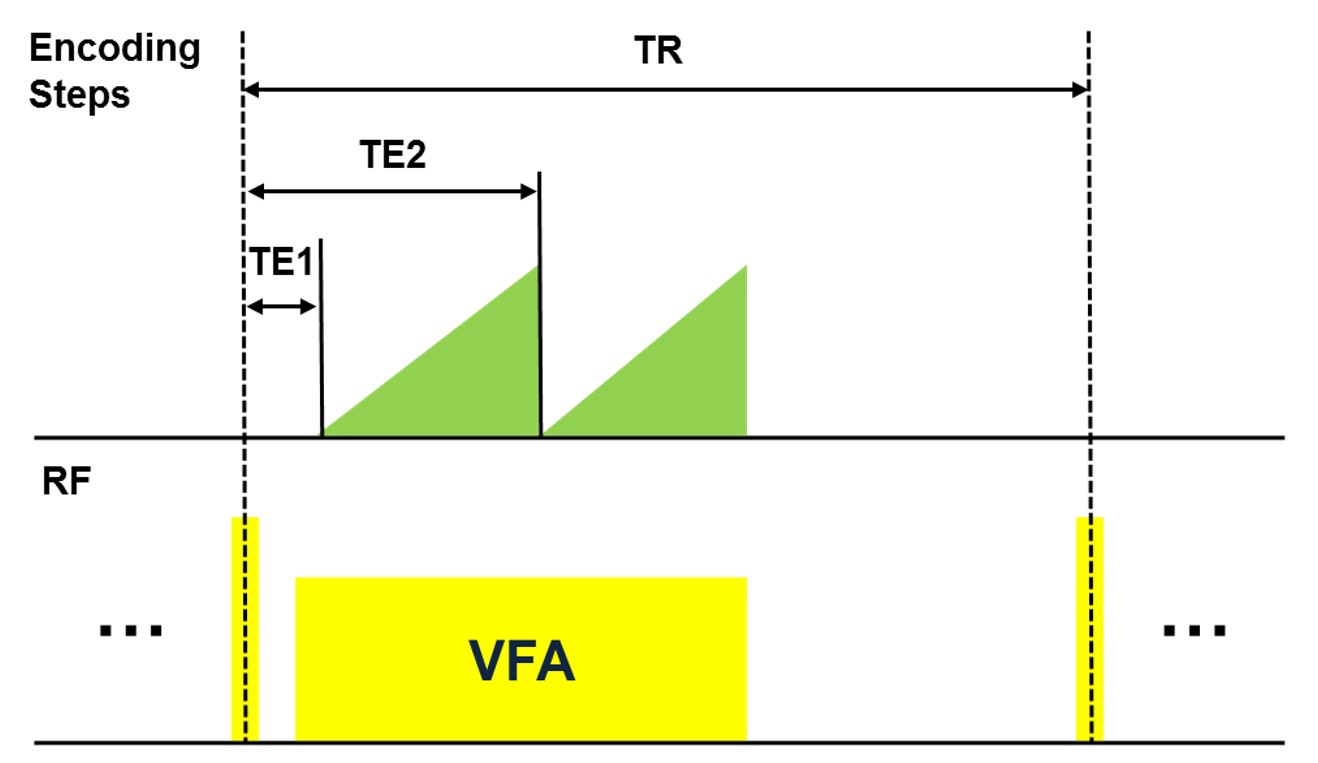
Pulse Sequence: The dVISTA sequence takes advantage of conventional variable flip angle (VFA) turbo spin echo sequence. T1/T2 contrast are obtained simultaneously by sampling k-space center using different echoes in one TR, as shown in Fig.1.
MR Protocol: All MR images were acquired on a 3.0T MR Scanner (Philips Achieva, Best, Netherlands). Imaging parameters of dVISTA included: FOV = 200 x 180 x 120 mm3, voxel size = 0.8 x 0.8 x 0.8 mm3, TR = 800 ms, TE = 22.5/180 ms, echo train length (ETL) = 68, scan time = 5:59. The VFA scheme were calculated using extended phase graph5,6 by setting minimum flip angle (FA) = 35° and maximum FA = 70°/90°. Furthermore, in order to validate the performance of dVISTA, T1-VISTA and T2-FLAIR were used to acquire reference T1/T2 images, respectively. For T1-VISTA, imaging parameters were: resolution = 0.8 x 0.8 x 0.8 mm3, TR = 800 ms, TE = 18.1 ms, echo train length (ETL) = 37, scan time = 5:37. For T2-FLAIR, imaging parameters were: resolution = 1.0 x 1.0 x 1.0 mm3, TR/TE/TI = 5000/340/1650 ms.
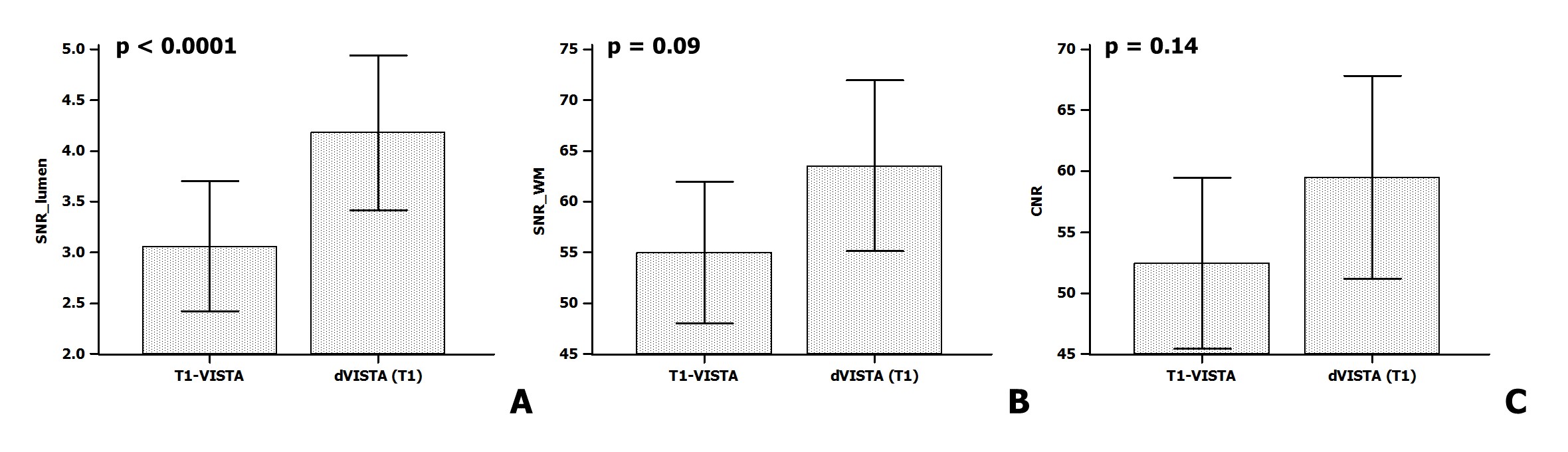
In-vivo validation: Three healthy volunteers and two CVT patients (female, 36 & 46 years) were recruited in this study. Informed consent was obtained from all participants. SNR of lumen/white matter (WM) and CNR, which is calculated by CNR = SNR_WM – SNR_lumen, were measured in healthy volunteers by taking six consecutive slices of superior sagittal sinus as regions of interest, and paired t-test was conducted to compare the performance of dVISTA and T1-VISTA. Additionally, two patients were scanned to explore T1/T2 signal properties of CVT and test the clinical feasibility of dVISTA.
RESULTS
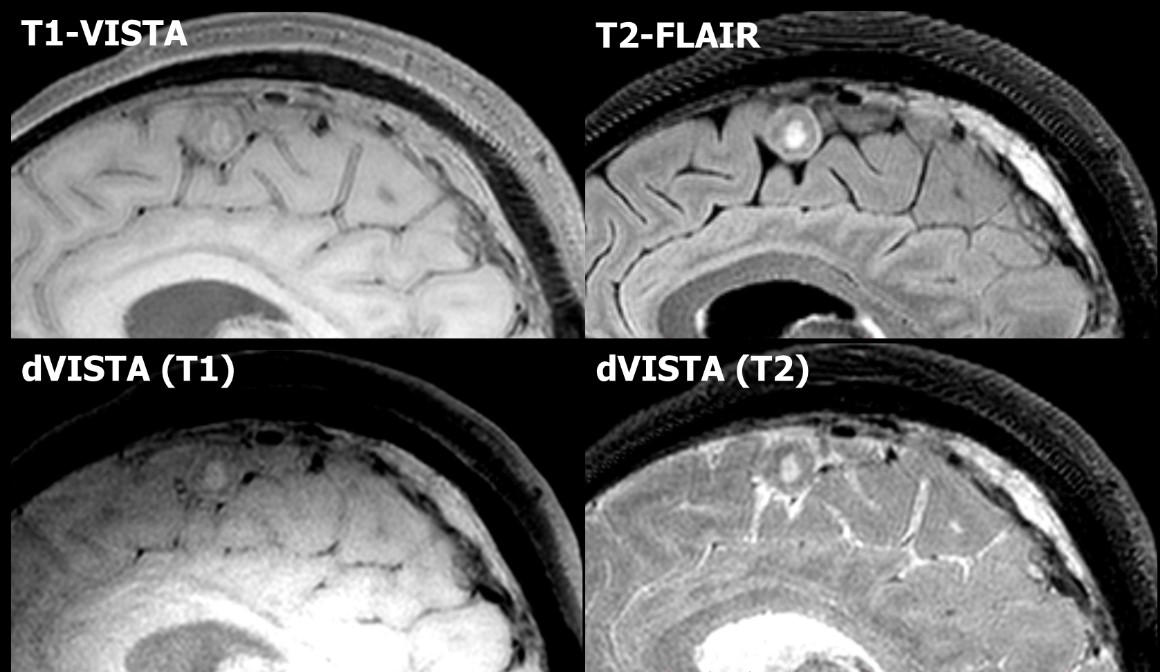
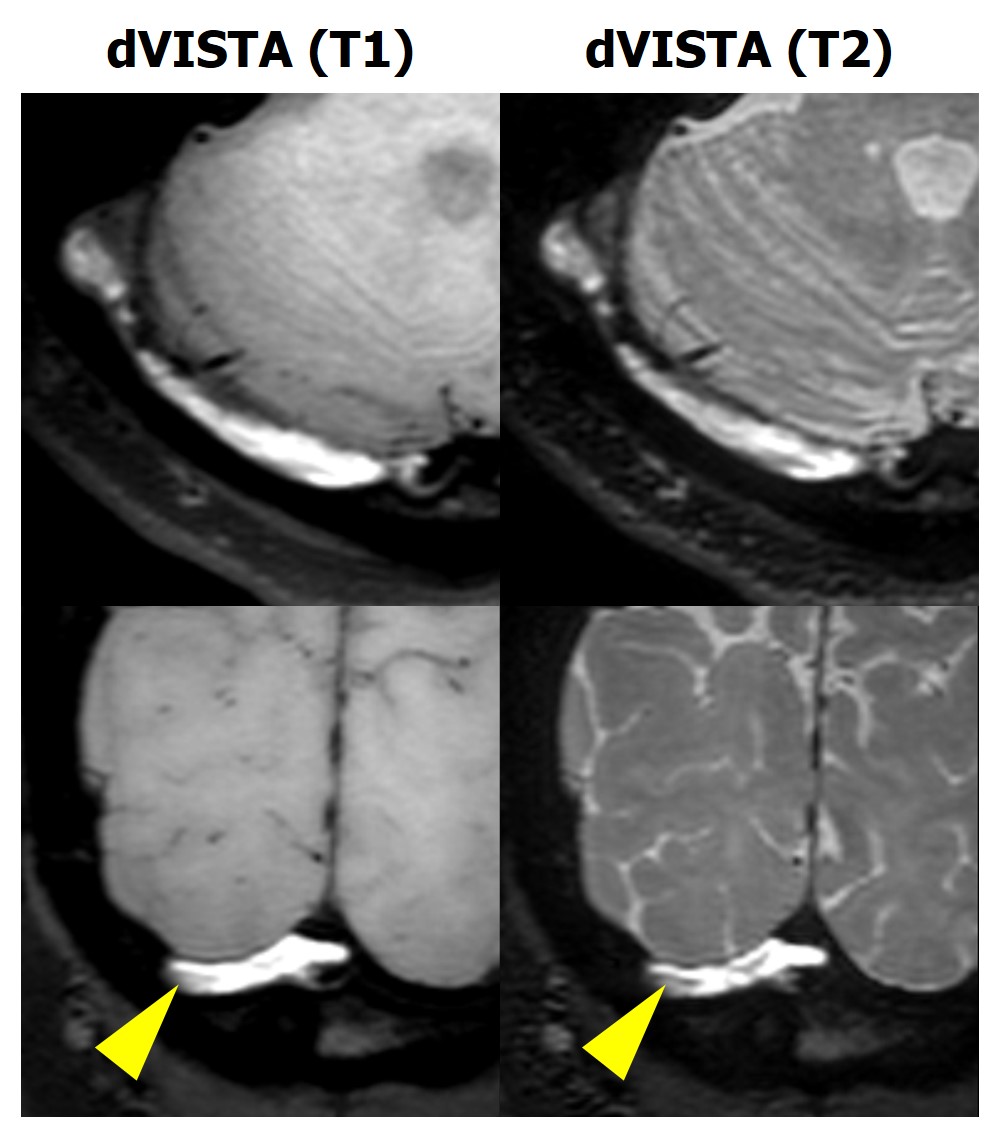
SNR and CNR measurements were summarized in Fig.2. Statistical results indicated that dVISTA can provide comparable SNR_WM and CNR as conventional T1-VISTA, and showed higher SNR_lumen than dVISTA. By investigating a 46-year-old female patient, as shown in Fig.3, CVT appears isointense signal in both T1-VISTA and dVISTA (T1), and hyperintense signal in both T2-FLAIR and dVISTA (T2), hinting that CVT was chronic. Fig.4 showed another CVT patient with both hyperintense signal in transverse sinus, indicating that CVT was in subacute stage. Within this thrombus, isointense signal in T1 images and iso/hypointense signal in T2 images was found, suggesting acute thrombus formation.DISCUSSION
In this study, we proposed a dual-contrast MR sequence, dVISTA, to detect and stage CVT within one scan. Volunteer studies showed that dVISTA can provide adequate image contrast as conventional T1/T2 imaging, and it is feasible to incorporate T2 contrast in conventional VISTA sequence without sacrifice image quality, which is proved by SNR/CNR measurements. Patients study demonstrated that T1/T2 signal properties varied with CVT progression, which validated the clinical feasibility of this study. Conventional imaging diagnosis of CVT requires a combination of T1/T2 weighted imaging and MR venography (MRV), resulting in a diagnostic delay in patients and suffering with diagnostic pitfalls7. Benefit from the intrinsic flow suppression properties of turbo spin echo, dVISTA can be utilized to jointly investigate CVT, venous sinus wall, arachnoid granulations and other surrounding tissues in one 6-min whole brain scan, which is time-efficient and immune to inter-scan motion.CONCLUSION
This study proposed a new MR imaging method for CVT staging by simultaneously acquiring T1 and T2-weighted images using dVISTA sequence, which has the potential to detect and differentiate thrombus in clinical routine.Acknowledgements
No acknowledgement found.References
1. Bousser MG, Ferro JM. Lancet Neurol. 2007;6:162–170.
2. Ferro JM, et al. Stroke. 2004;35:664–670.
3. Yang Q, et al. Stroke. 2015;47:404-409.
4. Anish B, Marek AM. Handbook of Neurocritical Care. Springer, 2011.
5. Qiao Y, et al. J Magn Reson Imaging. 2011;34:22-30.
6. Zhou ZC, et al. JCMR 2015;17:41.
7. Hinman JM, et al. European Journal of Radiology. 2002;41:147-152.
Figures