3086
Deep learning for prognosis in Degenerative cervical myelopathy1NeuroPoly Lab, Institute of Biomedical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Division of Neurosurgery, Departement of surgery, University of Toronto, Toronto, ON, Canada, 3Departement of surgery, McGill University, Montreal, QC, Canada, 4Functional Neuroimaging Unit, CRIUGM, Université de Montréal, Montreal, QC, Canada
Synopsis
Degenerative cervical myelopathy is an important cause of spinal cord dysfunction in adults worldwide 1,2. This study’s goal is to use boosting algorithm and deep learning on MRI and clinical data to predict the condition of a patient 6 months after baseline. Results show an improvement of prediction accuracy when combining MRI with clinical data (82.3%) versus with clinical data only (78.5%). The heterogeneity of the data makes it difficult for the learning algorithm to generalize, however future work exploiting boosting algorithm for structural data, and dimensionality reduction (e.g., via MRI feature extraction) could further improve prognosis accuracy.
Introduction
Degenerative Cervical Myelopathy (DCM) is characterized by a compression of the spinal cord, which implies a motor dysfunction for the patient.The prognosis of the patient is still very challenging due to the complex nature of the illness 1,2,5. While decompressive surgery remains an effective treatment, there are important risks associated with the procedure (e.g., dysphagia, pseudarthrosis, C5 palsy) 2. These risks warrant an accurate evaluation of each patient’s prognosis in order to decide about treatment. Current prognosis is based on clinical score and normalized compression measure 3, however this approach still has limited prognosis values 4. The goal of this study was to develop a neural network model that can predict motor scores at 6 months using baseline clinical scores and routine structural MRI.Methods
Demographics and Data acquisition: Data were prospectively acquired from 504 patients as part of the AOSpine database 6. Data consisted of clinical scores at baseline (mJOA, Nurick, NDI) and MRI data at baseline (sagittal, coronal and axial composed of T1 and T2 weighted scan). MRI quality and contrast largely varied within and across sites (see Figure 1), making it a realistic scenario for validating our proposed machine learning approach. All patients underwent decompressive surgery and clinical scores were re-obtained 6 months after surgery. The outcome measure used for the prediction was the modified Japanese Orthopaedic Association Scale (mJOA).
Data preprocessing: To select the clinical scores to use in the neural network model, a stepwise forward model was used to predict the ΔmJOA score (mJOA difference between baseline and 6-month). A k-nearest-neighbors (KNN) method was used to retrieve missing values in the database. To accommodate the algorithm due to the relatively low number of patients and the high heterogeneity, we aimed at predicting two functional outcome classes: ΔmJOA>2 (improvement) and ΔmJOA<2 (stable).
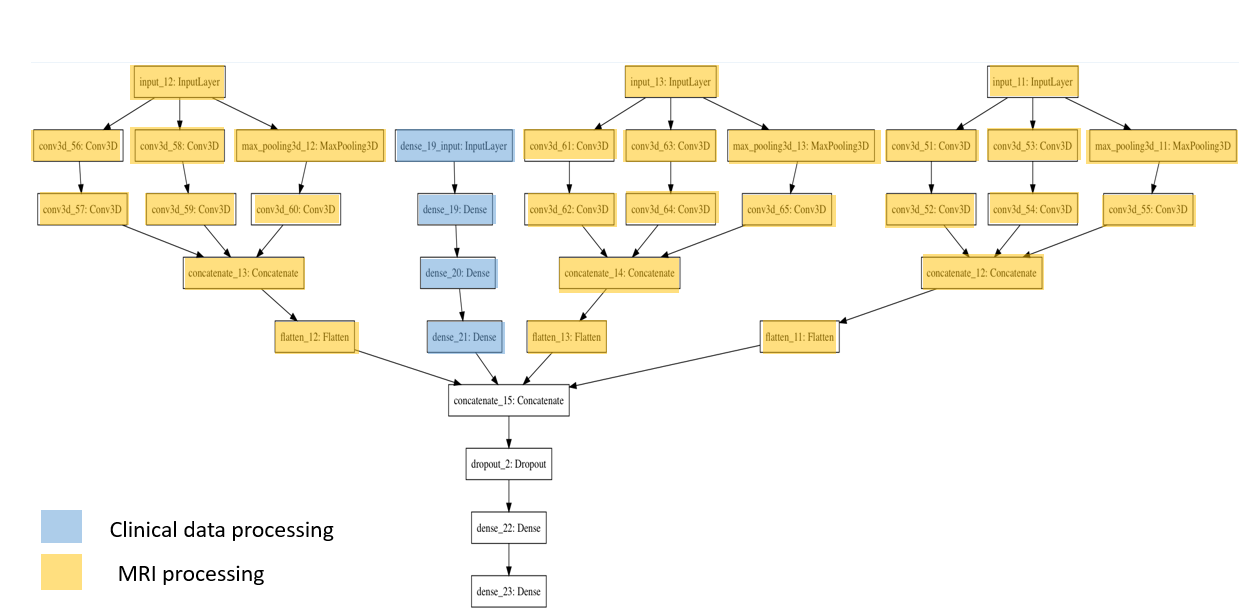
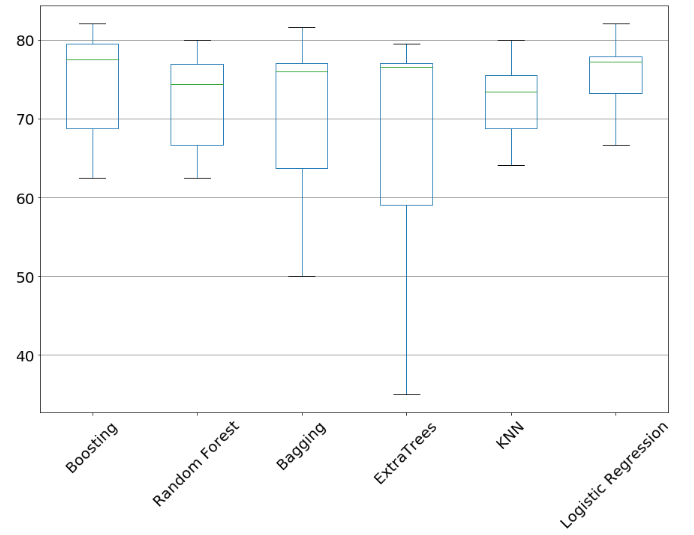
Training/evaluation of the model: First, we looked for the best prediction model based on the clinical data only (to be compared later with deep learning approaches). To this end, we evaluated several algorithms: boosting (xgboost with hyperparameter tuning through Bayesian optimization), random forest, bagging, extraTrees, KNN and logistic regression. Then, we looked at two deep learning architectures: (i) a traditional convolutional neural network (CNN) with multiple inputs (clinical data, axial, sagittal and coronal MRIs) and (ii) an InceptionNet 7-9, which structure is more adapted to multiple and inter-related inputs. The InceptionNet had three inception modules (axial, sagittal coronal MRI) and a separate branch for the clinical data, as illustrated in Figure 2. The implementation was done in Python and used the Keras library. The dataset was split into: 2/3 (training) and 1/3 (testing). Evaluation was done on the testing dataset using cross-validation.
Models were trained for 100 epochs with 100 steps and 50 validation steps. Each model was trained 20 times (each time with random initialization), in order to compute the mean accuracy (using Scikit-learn).
Results
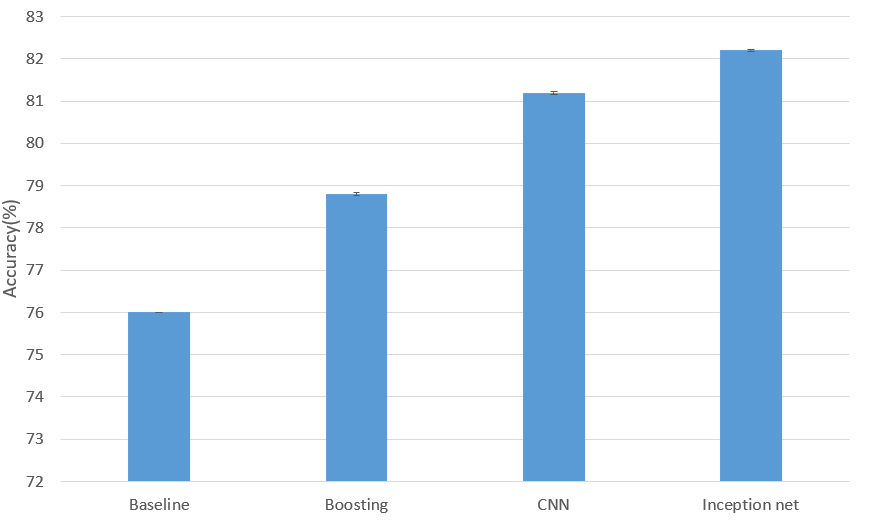
Amongst all algorithms compared to predict ΔmJOA on clinical data only, boosting yielded best results (see Figure 3). When considering both clinical and MRI data using deep learning approach, the InceptionNet got the best accuracy result (82.3 %, also see Figure 4). We noticed that the dataset is largely unbalanced because the baseline starts at 76% (instead of the theoretical 50%).Discussion/Conclusion
This study evaluated several classification models for predicting functional deficits 6 months after decompressive surgery on DCM patients. The InceptionNet produced an improvement of accuracy from 78.5% (when considering clinical data only) to 82.3% (when adding clinical MRIs). The improvement from baseline is currently limited, largely due to the heterogeneity and relatively small size of the dataset for such deep networks. Encouraging avenues to explore include reducing the dimensionality of the MRI input by selecting features such as cross-sectional area, cord shape or compression level (Martin et al. 2018).Acknowledgements
Funded by the Canada Research Chair in Quantitative Magnetic Resonance Imaging [950-230815], the Canadian Institute of Health Research [CIHR FDN-143263], the Canada Foundation for Innovation [32454, 34824], the Fonds de Recherche du Québec - Santé [28826], the Fonds de Recherche du Québec - Nature et Technologies [2015-PR-182754], the Natural Sciences and Engineering Research Council of Canada [435897-2013], the Canada First Research Excellence Fund (IVADO and TransMedTech) and the Quebec BioImaging Network [5886].References
1. Badhiwala, Jetan H., and Jefferson R. Wilson. 2018. “The Natural History of Degenerative Cervical Myelopathy.” Neurosurgery Clinics of North America 29 (1): 21–32.
2. Kato, So, and Michael Fehlings. 2016. “Degenerative Cervical Myelopathy.” Current Reviews in Musculoskeletal Medicine 9 (3): 263–71.
3. Fehlings, M. G., S. C. Rao, C. H. Tator, G. Skaf, P. Arnold, E. Benzel, C. Dickman, et al. 1999. “The Optimal Radiologic Method for Assessing Spinal Canal Compromise and Cord Compression in Patients with Cervical Spinal Cord Injury. Part II: Results of a Multicenter Study.” Spine 24 (6): 605–13.
4. Martin, Allan R., Benjamin De Leener, Julien Cohen-Adad, Sukhvinder Kalsi-Ryan, David W. Cadotte, Jefferson R. Wilson, Lindsay Tetreault, et al. 2018. “Monitoring for Myelopathic Progression with Multiparametric Quantitative MRI.” PloS One 13 (4): e0195733.
5. Fehlings, Michael G. 2018. “Current Knowledge in Degenerative Cervical Myelopathy.” Neurosurgery Clinics of North America 29 (1): xiii – xiv.
6. Kato, So, Aria Nouri, Dongjin Wu, Satoshi Nori, Lindsay Tetreault, and Michael G. Fehlings. 2017. “Comparison of Anterior and Posterior Surgery for Degenerative Cervical Myelopathy: An MRI-Based Propensity-Score-Matched Analysis Using Data from the Prospective Multicenter AOSpine CSM North America and International Studies.” The Journal of Bone and Joint Surgery. American Volume 99 (12): 1013–21.
7. Raj, Bharath. 2018. “A Simple Guide to the Versions of the Inception Network.” Towards Data Science. Towards Data Science. May 29, 2018. https://towardsdatascience.com/a-simple-guide-to-the-versions-of-the-inception-network-7fc52b863202.
8. Sharma, Neha, Vibhor Jain, and Anju Mishra. 2018. “An Analysis Of Convolutional Neural Networks For Image Classification.” Procedia Computer Science 132 (January): 377–84.
9. Szegedy, Christian, Wei Liu, Yangqing Jia, Pierre Sermanet, Scott Reed, Dragomir Anguelov, Dumitru Erhan, Vincent Vanhoucke, and Andrew Rabinovich. 2014. “Going Deeper with Convolutions.” arXiv [cs.CV]. arXiv. http://arxiv.org/abs/1409.4842.
Figures