3080
Radiomics Approach for Prediction of Tumor Recurrence and Progression of Skull Base Meningioma1Section of Neuroradiology, Department of Medical Imaging, Chi-Mei Medical Center, Tainan, Taiwan, 2Department of Radiological Sciences, University of California, Irvine, CA, United States, 3Department of Radiology, E-Da Hospital and I-Shou University, Kaohsiung, Taiwan
Synopsis
A subset of low grade skull base meningiomas (SBM) shows early progression/recurrence (P/R). In clinical practice, one of the main challenges in the treatment of SBM is to determine factors that correlate with P/R. This study investigated the role of radiomics for the prediction of P/R. Sixty patients diagnosed with benign SBM were studied. Totally 99 descriptors were extracted from the various MR sequences. The prediction accuracy of P/R was 90% and the AUC of the prediction model was 0.94. Our study also noted that subsequent P/R of SBM after surgery was not associated with the completeness of tumor resection.
Background and Purpose
Approximate 20–30% of meningiomas grow
in the skull base [1]. Although the majority of skull base
meningiomas (SBM) are low grade (WHO grade I), a subset of WHO grade I SBM
shows early progression/recurrence (P/R) in the first year after surgical
resection [2]. Because of the complex anatomic
structures in skull base, complete surgical resection of the tumor (Simpson
Grade I-III resection) is often difficult to achieve safely [3]. SBMs are often associated with
involvement of complex neurovascular structures and brainstem compared with
lesions not arising from the skull base, conservative follow up or subtotal tumor
resection (STR) to avoid subsequent surgical complications are also the
treatment of choice [4]. In clinical practice, one of the main challenges in
the treatment of SBM is to determine factors that correlate with P/R. The
conventional qualitative MR imaging findings such as mushroom shape, bone
osteolysis, dural tail, and proximity to major sinuses had been reported as the
important variables related to P/R [2].
Recently, the association of apparent diffusion coefficient (ADC) and P/R has
been reported by our group [5]. Besides ADC, it is very likely that other
quantitative imaging parameters may also be associated with tumor recurrence.
Thus, in this study, we further investigated the role of radiomics for the
prediction of P/R.
Materials and Methods
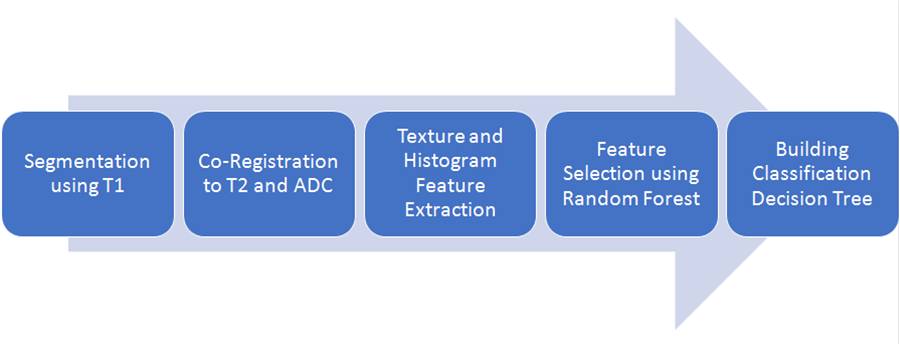
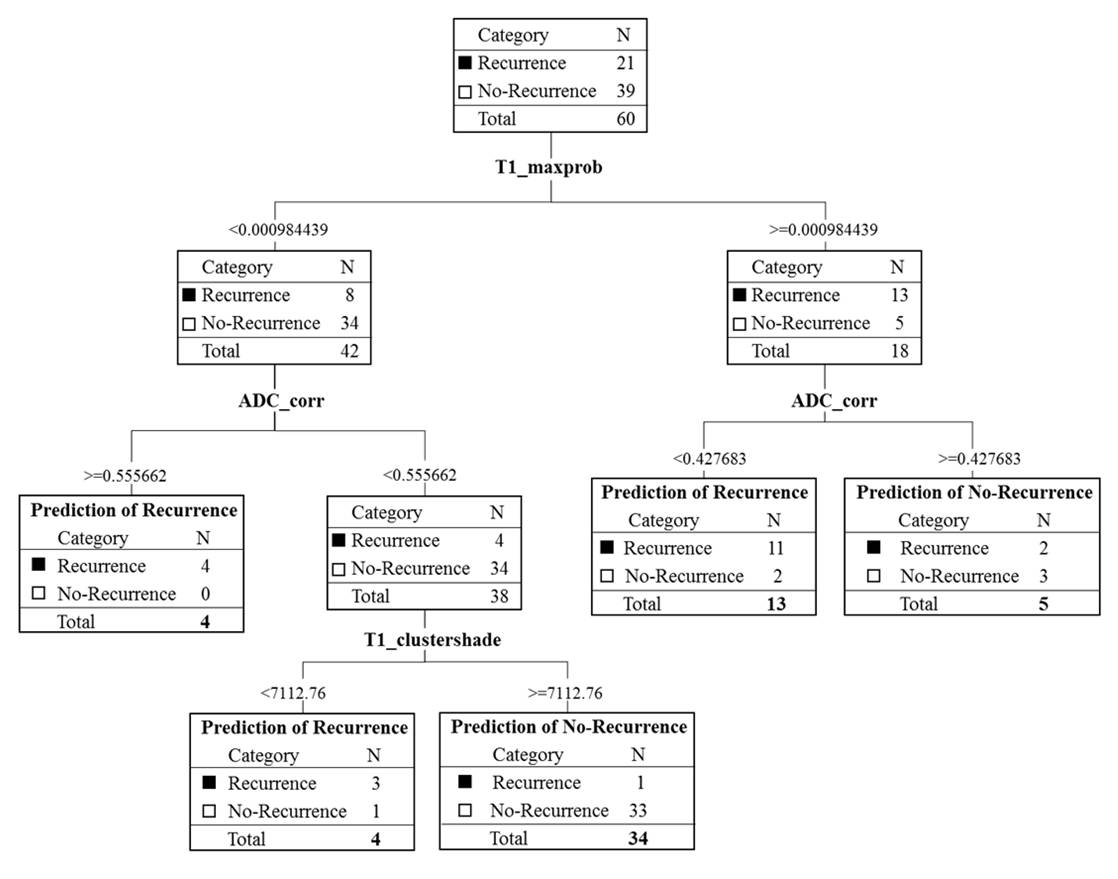
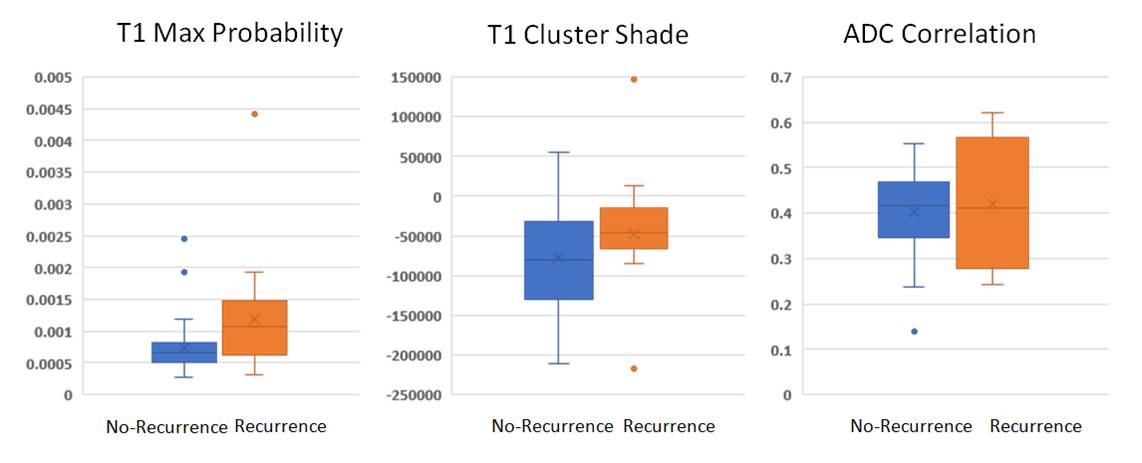
Sixty patients (age 26–75 years; median age, 56 years) included in this study were diagnosed with low grade (WHO grade I) SBM by MRI and pathological confirmation. The median follow-up time was 41 months (range 12-115 months), and a total of 21 patients were found to have recurrence or progression, and 39 patients remained disease-free or without any sign of progression. The MRI images were acquired using a 1.5T or a 3.0T scanner. The protocols of MR imaging included axial and sagittal spin echo T1-weighted imaging (T1WI), fast spin-echo T2-weighted imaging (T2WI), fluid attenuated inversion recovery (FLAIR), T2*-weighted gradient-recalled echo (GRE), contrast-enhanced (CE) T1WI in axial and coronal sections, and diffusion weighted imaging (DWI). Figure 1 shows the flowchart of the analysis process. The lesion was segmented from subtracted contrast enhancement images. For each lesion, the operator placed an initial region of interest (ROI) indicating the lesion location, and also decided the beginning and ending slices that contained the lesion. Then the outline of the lesion ROI on each imaging slice was automatically obtained using the fuzzy c-means (FCM) clustering based algorithm [6]. The ROIs from all imaging slices containing this lesion were combined to obtain 3D information of the whole lesion. Then 3D connected-component labeling was applied to remove scattered voxels not connecting to the main lesion ROI, and hole-filling to include all voxels contained within the main ROI which were labeled as non-lesion. The segmented tumor mask was co-registered to T2W images and ADC map to localize the tumor location on corresponding images using affine transformation. This process was done by FLIRT. Within segmented tumor on enhanced T1W images, T2W images and ADC maps, 13 histogram features and 20 textural GLCM features were extracted on each modality [7]. Thus, totally we obtained 99 descriptors. To evaluate the importance of these features in differentiate patients with and without recurrence, random forest algorithms were utilized via Bootstrap-aggregated decision trees [8]. Three features, including T1 Max Probability, T1 Cluster Shade, ADC Correlation, with the highest importance were selected to build a decision tree with 5 leaves that makes coarse distinction between classes. The total number of split was 4 (Figure 2). This procedure was implemented in Matlab 2018b.Results
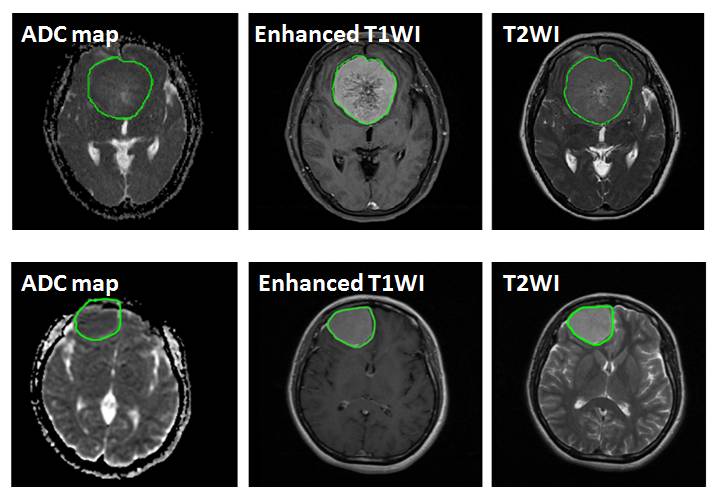
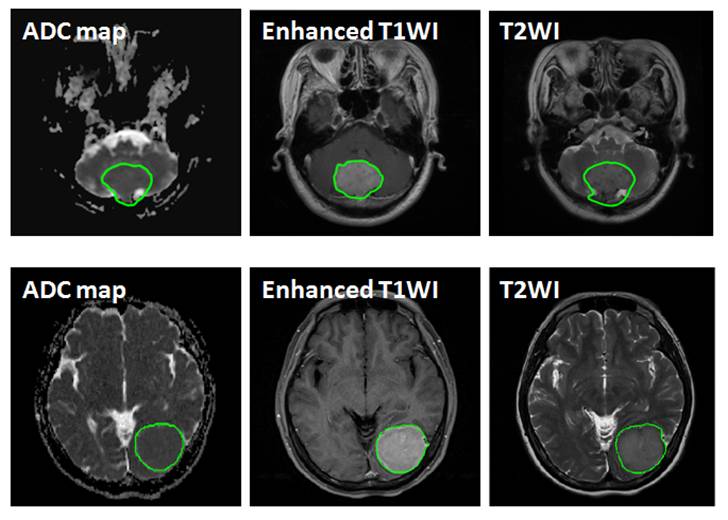
Of the 60 patients, 37 had complete tumor resection (Simpson Grade I-III) and 23 had incomplete tumor resection (Simpson Grade IV and V). Figure 3 shows two patients with Simpson Grade 2 with complete tumor resection in surgery: one had recurrence and the other did not in subsequent follow-up. Figure 4 shows another two patients with Simpson Grade 4 with incomplete tumor resection in surgery: one had progression and the other did not in subsequent follow-up. Figure 5 shows box plot for three features which were extracted from random forest algorithm and included in the final prediction model. The final classification results showed 18 true positive cases, 36 true negative cases, 3 false positive cases, and 3 false negative cases. The overall prediction accuracy is 90% and the AUC of the prediction model is 0.94. We also analyzed the impact of tumor resection completeness based on Simpson Grades, and found that it was not a risk factor associated with the progression/recurrence.Discussion
This study attempted to use radiomics approach in limited cases of skull base meningioma for the prediction of tumor recurrence or progression after surgery. Our results showed that, with total 99 descriptors of histogram features and textural GLCM features extracted from segmented tumor on enhanced T1W images, T2W images and ADC maps, a prediction accuracy of 90% and an AUC of 0.94 of the prediction model were achieved. The results were better than our previous work merely using ADC, which was measured by operator-defined ROIs, as the predictor [5].Acknowledgements
This study was supported in part by NIH R01 CA127927.References
[1] Mansouri A, et al. Surgically resected skull base meningiomas demonstrate a divergent postoperative recurrence pattern compared with non–skull base meningiomas. J Neurosurg 2016;125:431–40.; [2] Ildan F, et al. Predicting the probability of meningioma recurrence in the preoperative and early postoperative period: a multivariate analysis in the midterm follow-up. Skull Base. 2007;17:157–71.; [3] Simpson D. The recurrence of intracranial meningiomas after surgical treatment J Neurol Neurosurg Psychiatr. 1957;20:22–39.; [4] Sekhar LN, et al. Skull base meningiomas: aggressive resection. Neurosurgery. 2015; 62 Suppl 1: 30–49.; [5]. Ko CC, et al. Applications of diffusion-weighted MR imaging in brain tumors. J Neurooncol. 2018;138(1):63-71.; [6] Nie K, et al. Quantitative analysis of lesion morphology and texture features for diagnostic prediction in breast MRI. Academic Radiology. 2008;15(12):1513-25.; [7] Haralick RM, et al. Textural features for image classification. IEEE Transactions on Systems, Man, and Cybernetics. 1973(6):610-21.; [8] Segal MR. Machine learning benchmarks and random forest regression. Center for Bioinformatics & Molecular Biostatistics. 2004.Figures